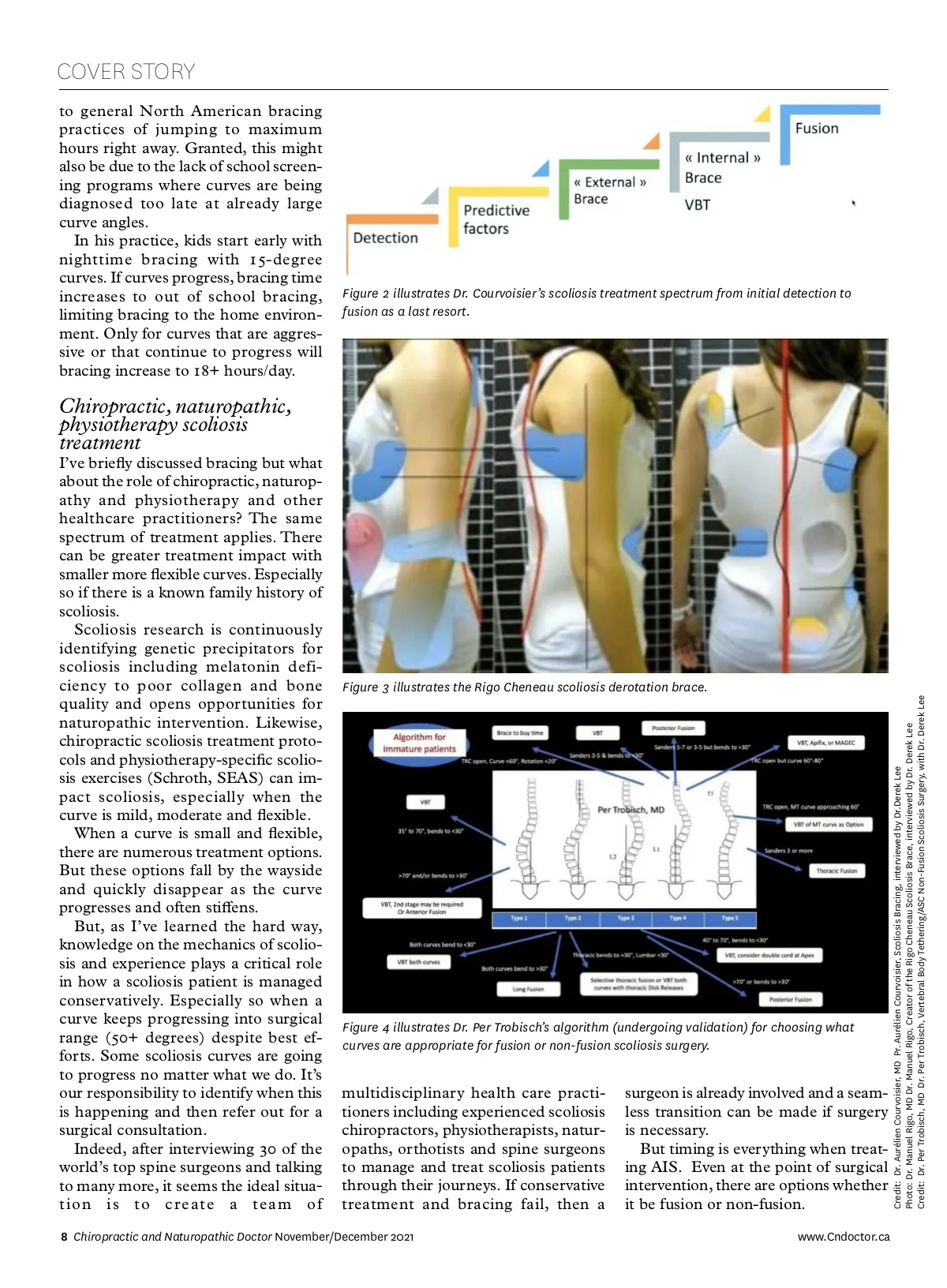
Figure 4 illustrates the ongoing need for conservative scoliosis healthcare. Surgical scoliosis options: fusion and non-fusion Spine surgeons are not created equal. Just like chiropractors, naturopaths and physiotherapists, we all vary in skill sets and levels of expertise and experi-ence. The same is true for spine sur-geons. One hundred percent of spine surgeons can offer fusion surgery to correct scoliosis. On the other hand, only a small percentage of spine sur-geons, around 5-10%, are currently capable of offering non-fusion scoliosis surgery. In all of Canada, approxi-mately 10 orthopedic spine surgeons offer both non-fusion and fusion scoli-osis surgery. Fusion surgery for scoliosis involves inserting screws into vertebral pedicles posteriorly and attaching correspond-ing metal rods. The spine is de-rotated and a normal sagittal alignment is at-tempted. Bone chips are added to the exposed posterior column and the spine fuses as one mass for the length of instrumentation. Although this is currently the gold standard for scoliosis surgery, adjacent segment degeneration (ASD) is com-mon above and below the fused levels leading to faster disc and facet joint degeneration. This is much more com-mon for lumbar fusions especially as levels are fused toward the sacrum as lumbar spine flexibility is lost. This may necessitate additional fusions to stabilize levels that have degenerated. Thoracic only fusions have a better long-term track record with less ASD due to the inherent stiffness of this part of the spine. A relatively new surgical procedure, which does not involve fusion, called Vertebral Body Tethering (VBT), in-volves inserting screws anterolateral www.Cndoctor.ca into the vertebrae along the convex side of the scoliosis curve. A polyethylene cord or tether is attached to the screw heads and tensioned thereby straight-ening the curve typically by 50%. Ad-ditional straightening of the curve is seen with continued passive growth of the spine to maturity. At maturity, bone growth modulation of the vertebrae will stabilize the tethered levels. The goal of this non-fusion technique is to avoid fusion. Revision rates are 10-15% due to tether ruptures and or overcor-rection of the curve if the adolescent grows too quickly. When a scoliosis non-fusion/fusion surgeon is part of the team early on, then that surgeon may have non-fusion surgical options available like VBT which are appropriate, in general, for adolescents during their growth spurts. Anterior Scoliosis Correction (ASC) is generally extending VBT to mature spines that have reached maturity. Once you understand scoliosis, you can reverse engineer countermeasures and develop conservative and surgical treat-ment options. Then, you can match appropriate treatment options with specific patient maturity levels and sco-liosis curve(s) severity to form a reason-ably effective treatment plan. As Dr. Courvoisier mentioned, he proposes a “comprehensive” approach to treating scoliosis with conservative treatment on one end and surgical in-tervention at the other end of the spectrum. Even this approach is not widely implemented for scoliosis care although it should be. But, taking this a step farther, scoli-osis management doesn’t just stop after the spine stops growing and matures. Management of scoliosis doesn’t stop post bracing or post-surgery whether it be non-fusion or fusion. Side effects of scoliosis Indeed, there is a multitude of side ef-fects that ripple from the spinal curves impacted by scoliosis. The lumbar and cervical spines are typically impacted with the loss of cervical spine lordosis that often reverses into kyphosis. Early cervical and lumbar disc degeneration can often be seen in adolescents. Once again, regardless of conservative treatment including bracing or surgical intervention, these spinal junction areas need care. This is an obvious opportu-nity for chiropractors, naturopaths and physiotherapists to work on posture, spine flexibility, strength and nutrition on an ongoing basis. Conclusion Understanding Scoliosis Credit: Dr. Derek Lee, DC,RAc https://www.youtube.com/c/DerekLee Ideally, I’d like to see a multidiscipli-nary team of healthcare practitioners bring their specific skills and experi-ence at the right time on the treatment spectrum. Surgeons are integrated at detection but monitoring, especially through the adolescent growth spurt to intervene if conservative treatment fails with both non-fusion and fusion surgi-cal options. Right now, scoliosis treatment is mostly narrow in breadth, discon-nected among disciplines and confus-ing for parents, patients and healthcare practitioners to navigate. There is much work to do, but a comprehensive multidisciplinary approach to manag-ing and treating scoliosis is more than worth the effort. Read Dr. Lee's previous article about scoliosis at cndoctor.ca/navigating-scoliosis/ November/December 2021 Chiropractic and Naturopathic Doctor 9
Chiropractic + Naturopathic Doctor November/December 2021: Page 9