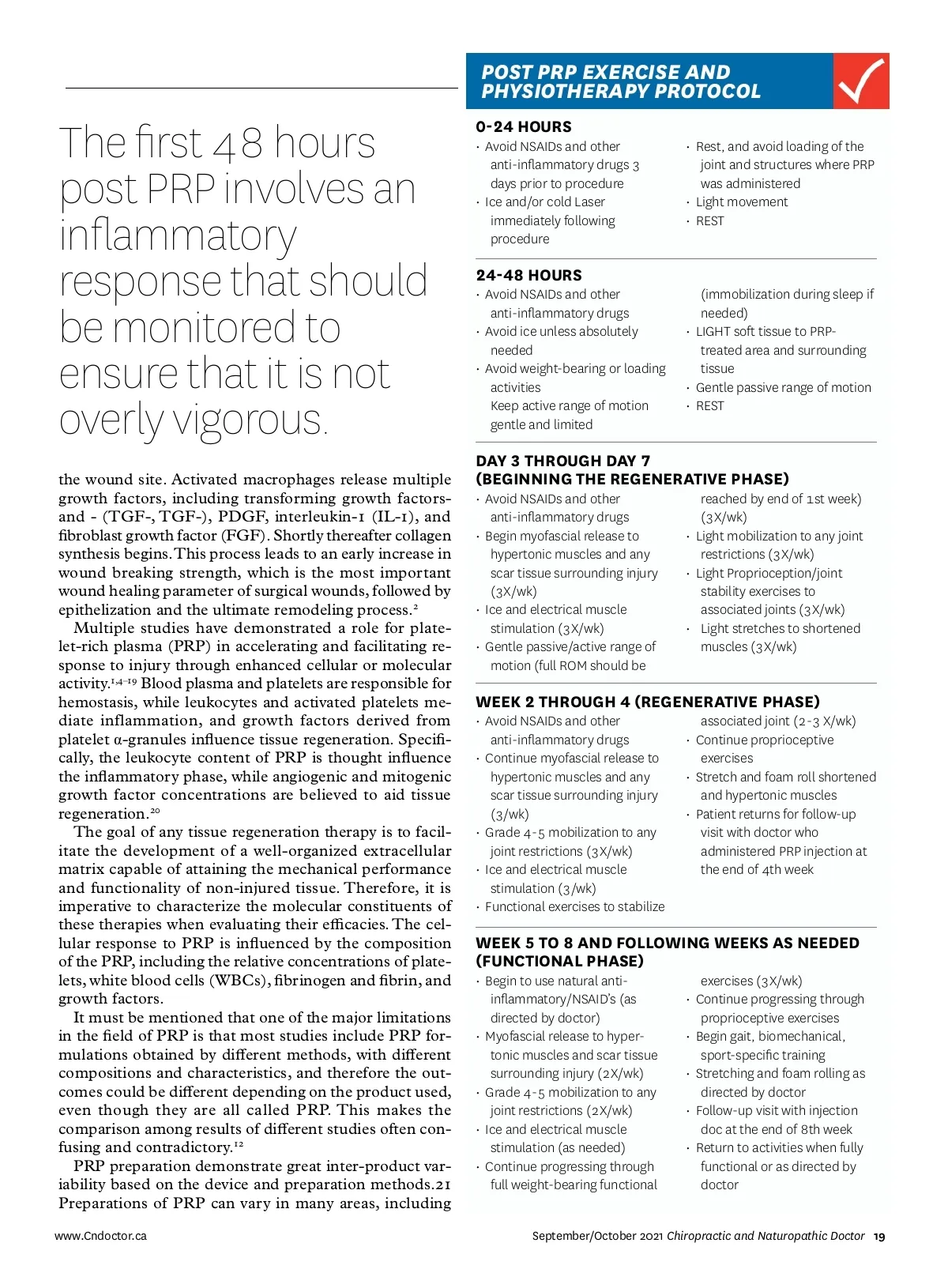
POST PRP EXERCISE AND PHYSIOTHERAPY PROTOCOL The first 48 hours post PRP involves an inflammatory response that should be monitored to ensure that it is not overly vigorous. the wound site. Activated macrophages release multiple growth factors, including transforming growth factors-and -(TGF-, TGF-), PDGF, interleukin-1 (IL-1), and fibroblast growth factor (FGF). Shortly thereafter collagen synthesis begins. This process leads to an early increase in wound breaking strength, which is the most important wound healing parameter of surgical wounds, followed by epithelization and the ultimate remodeling process. 2 Multiple studies have demonstrated a role for plate-let-rich plasma (PRP) in accelerating and facilitating re-sponse to injury through enhanced cellular or molecular activity. 1,4–19 Blood plasma and platelets are responsible for hemostasis, while leukocytes and activated platelets me-diate inflammation, and growth factors derived from platelet α -granules influence tissue regeneration. Specifi-cally, the leukocyte content of PRP is thought influence the inflammatory phase, while angiogenic and mitogenic growth factor concentrations are believed to aid tissue regeneration. 20 The goal of any tissue regeneration therapy is to facil-itate the development of a well-organized extracellular matrix capable of attaining the mechanical performance and functionality of non-injured tissue. Therefore, it is imperative to characterize the molecular constituents of these therapies when evaluating their efficacies. The cel-lular response to PRP is influenced by the composition of the PRP, including the relative concentrations of plate-lets, white blood cells (WBCs), fibrinogen and fibrin, and growth factors. It must be mentioned that one of the major limitations in the field of PRP is that most studies include PRP for-mulations obtained by different methods, with different compositions and characteristics, and therefore the out-comes could be different depending on the product used, even though they are all called PRP. This makes the comparison among results of different studies often con-fusing and contradictory. 12 PRP preparation demonstrate great inter-product var-iability based on the device and preparation methods.21 Preparations of PRP can vary in many areas, including www.Cndoctor.ca 0-24 HOURS • Avoid NSAIDs and other anti-inflammatory drugs 3 days prior to procedure • Ice and/or cold Laser immediately following procedure • Rest, and avoid loading of the joint and structures where PRP was administered • Light movement • REST 24-48 HOURS • Avoid NSAIDs and other anti-inflammatory drugs • Avoid ice unless absolutely needed • Avoid weight-bearing or loading activities Keep active range of motion gentle and limited (immobilization during sleep if needed) • LIGHT soft tissue to PRP-treated area and surrounding tissue • Gentle passive range of motion • REST DAY 3 THROUGH DAY 7 (BEGINNING THE REGENERATIVE PHASE) • Avoid NSAIDs and other anti-inflammatory drugs • Begin myofascial release to hypertonic muscles and any scar tissue surrounding injury (3X/wk) • Ice and electrical muscle stimulation (3X/wk) • Gentle passive/active range of motion (full ROM should be reached by end of 1st week) (3X/wk) • Light mobilization to any joint restrictions (3X/wk) • Light Proprioception/joint stability exercises to associated joints (3X/wk) • Light stretches to shortened muscles (3X/wk) WEEK 2 THROUGH 4 (REGENERATIVE PHASE) • Avoid NSAIDs and other anti-inflammatory drugs • Continue myofascial release to hypertonic muscles and any scar tissue surrounding injury (3/wk) • Grade 4-5 mobilization to any joint restrictions (3X/wk) • Ice and electrical muscle stimulation (3/wk) • Functional exercises to stabilize associated joint (2-3 X/wk) • Continue proprioceptive exercises • Stretch and foam roll shortened and hypertonic muscles • Patient returns for follow-up visit with doctor who administered PRP injection at the end of 4th week WEEK 5 TO 8 AND FOLLOWING WEEKS AS NEEDED (FUNCTIONAL PHASE) • Begin to use natural anti-inflammatory/NSAID’s (as directed by doctor) • Myofascial release to hyper-tonic muscles and scar tissue surrounding injury (2X/wk) • Grade 4-5 mobilization to any joint restrictions (2X/wk) • Ice and electrical muscle stimulation (as needed) • Continue progressing through full weight-bearing functional exercises (3X/wk) • Continue progressing through proprioceptive exercises • Begin gait, biomechanical, sport-specific training • Stretching and foam rolling as directed by doctor • Follow-up visit with injection doc at the end of 8th week • Return to activities when fully functional or as directed by doctor September/October 2021 Chiropractic and Naturopathic Doctor 19
Chiropractic + Naturopathic Doctor September/October 2021: Page 19