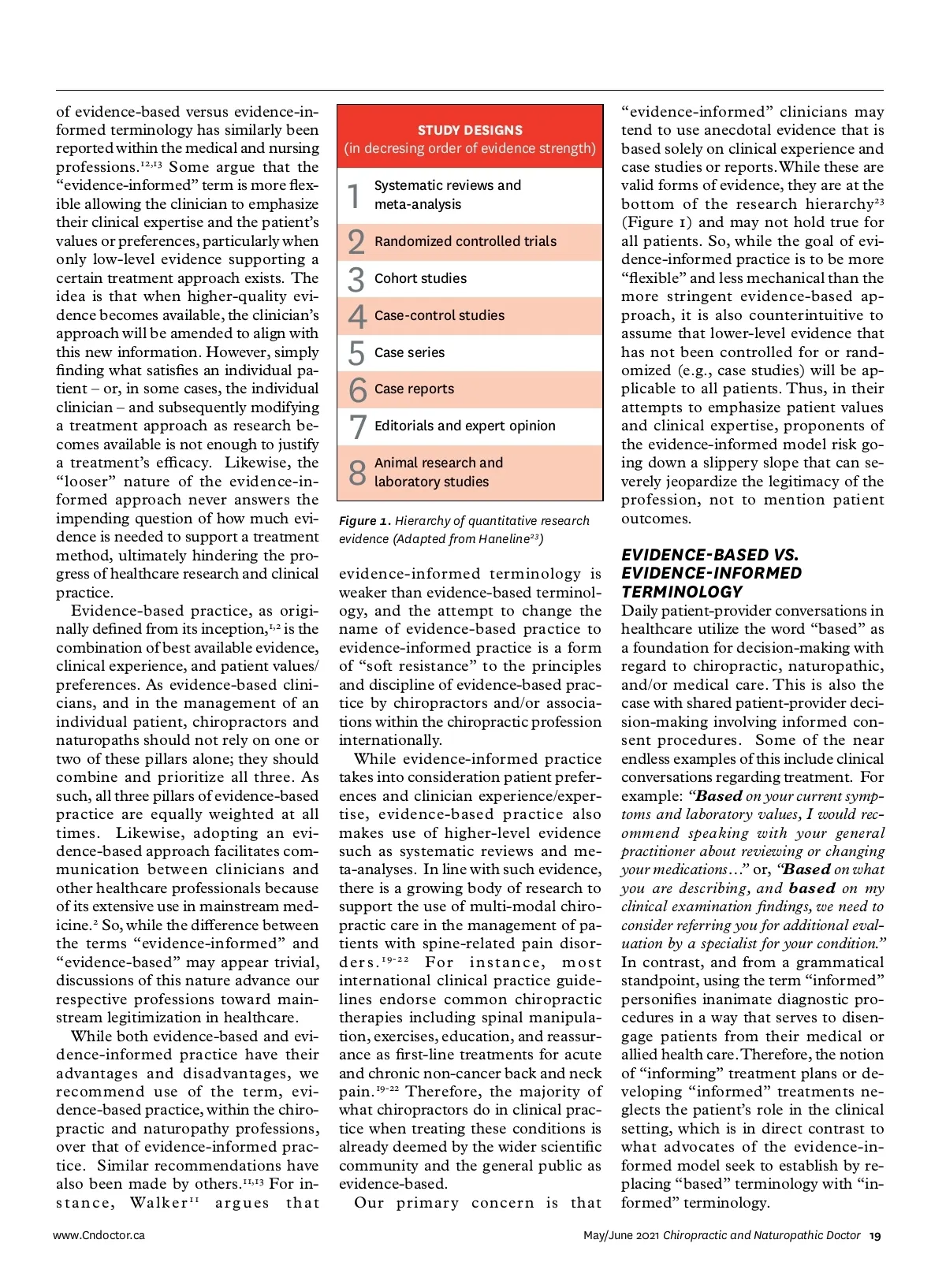
of evidence-based versus evidence-in-formed terminology has similarly been reported within the medical and nursing professions. 12,13 Some argue that the “evidence-informed” term is more flex-ible allowing the clinician to emphasize their clinical expertise and the patient’s values or preferences, particularly when only low-level evidence supporting a certain treatment approach exists. The idea is that when higher-quality evi-dence becomes available, the clinician’s approach will be amended to align with this new information. However, simply finding what satisfies an individual pa-tient – or, in some cases, the individual clinician – and subsequently modifying a treatment approach as research be-comes available is not enough to justify a treatment’s efficacy. Likewise, the “looser” nature of the evidence-in-formed approach never answers the impending question of how much evi-dence is needed to support a treatment method, ultimately hindering the pro-gress of healthcare research and clinical practice. Evidence-based practice, as origi-nally defined from its inception, 1,2 is the combination of best available evidence, clinical experience, and patient values/ preferences. As evidence-based clini-cians, and in the management of an individual patient, chiropractors and naturopaths should not rely on one or two of these pillars alone; they should combine and prioritize all three. As such, all three pillars of evidence-based practice are equally weighted at all times. Likewise, adopting an evi-dence-based approach facilitates com-munication between clinicians and other healthcare professionals because of its extensive use in mainstream med-icine. 2 So, while the difference between the terms “evidence-informed” and “evidence-based” may appear trivial, discussions of this nature advance our respective professions toward main-stream legitimization in healthcare. While both evidence-based and evi-dence-informed practice have their advantages and disadvantages, we recommend use of the term, evi-dence-based practice, within the chiro-practic and naturopathy professions, over that of evidence-informed prac-tice. Similar recommendations have also been made by others. 11,13 For in-stance, Walker 11 argues that www.Cndoctor.ca STUDY DESIGNS (in decresing order of evidence strength) 1 2 3 4 5 6 7 8 Systematic reviews and meta-analysis Randomized controlled trials Cohort studies Case-control studies Case series Case reports Editorials and expert opinion Animal research and laboratory studies Figure 1. Hierarchy of quantitative research evidence (Adapted from Haneline 23 ) “evidence-informed” clinicians may tend to use anecdotal evidence that is based solely on clinical experience and case studies or reports. While these are valid forms of evidence, they are at the bottom of the research hierarchy 23 (Figure 1) and may not hold true for all patients. So, while the goal of evi-dence-informed practice is to be more “flexible” and less mechanical than the more stringent evidence-based ap-proach, it is also counterintuitive to assume that lower-level evidence that has not been controlled for or rand-omized (e.g., case studies) will be ap-plicable to all patients. Thus, in their attempts to emphasize patient values and clinical expertise, proponents of the evidence-informed model risk go-ing down a slippery slope that can se-verely jeopardize the legitimacy of the profession, not to mention patient outcomes. evidence-informed terminology is weaker than evidence-based terminol-ogy, and the attempt to change the name of evidence-based practice to evidence-informed practice is a form of “soft resistance” to the principles and discipline of evidence-based prac-tice by chiropractors and/or associa-tions within the chiropractic profession internationally. While evidence-informed practice takes into consideration patient prefer-ences and clinician experience/exper-tise, evidence-based practice also makes use of higher-level evidence such as systematic reviews and me-ta-analyses. In line with such evidence, there is a growing body of research to support the use of multi-modal chiro-practic care in the management of pa-tients with spine-related pain disor-ders. 19-22 For instance, most international clinical practice guide-lines endorse common chiropractic therapies including spinal manipula-tion, exercises, education, and reassur-ance as first-line treatments for acute and chronic non-cancer back and neck pain. 19-22 Therefore, the majority of what chiropractors do in clinical prac-tice when treating these conditions is already deemed by the wider scientific community and the general public as evidence-based. Our primary concern is that Daily patient-provider conversations in healthcare utilize the word “based” as a foundation for decision-making with regard to chiropractic, naturopathic, and/or medical care. This is also the case with shared patient-provider deci-sion-making involving informed con-sent procedures. Some of the near endless examples of this include clinical conversations regarding treatment. For example: “ Based on your current symp-toms and laboratory values, I would rec-ommend speaking with your general practitioner about reviewing or changing your medications…” or, “ Based on what you are describing, and based on my clinical examination findings, we need to consider referring you for additional eval-uation by a specialist for your condition.” In contrast, and from a grammatical standpoint, using the term “informed” personifies inanimate diagnostic pro-cedures in a way that serves to disen-gage patients from their medical or allied health care. Therefore, the notion of “informing” treatment plans or de-veloping “informed” treatments ne-glects the patient’s role in the clinical setting, which is in direct contrast to what advocates of the evidence-in-formed model seek to establish by re-placing “based” terminology with “in-formed” terminology. EVIDENCE-BASED VS. EVIDENCE-INFORMED TERMINOLOGY May/June 2021 Chiropractic and Naturopathic Doctor 19
Chiropractic + Naturopathic Doctor May/June 2021: Page 19