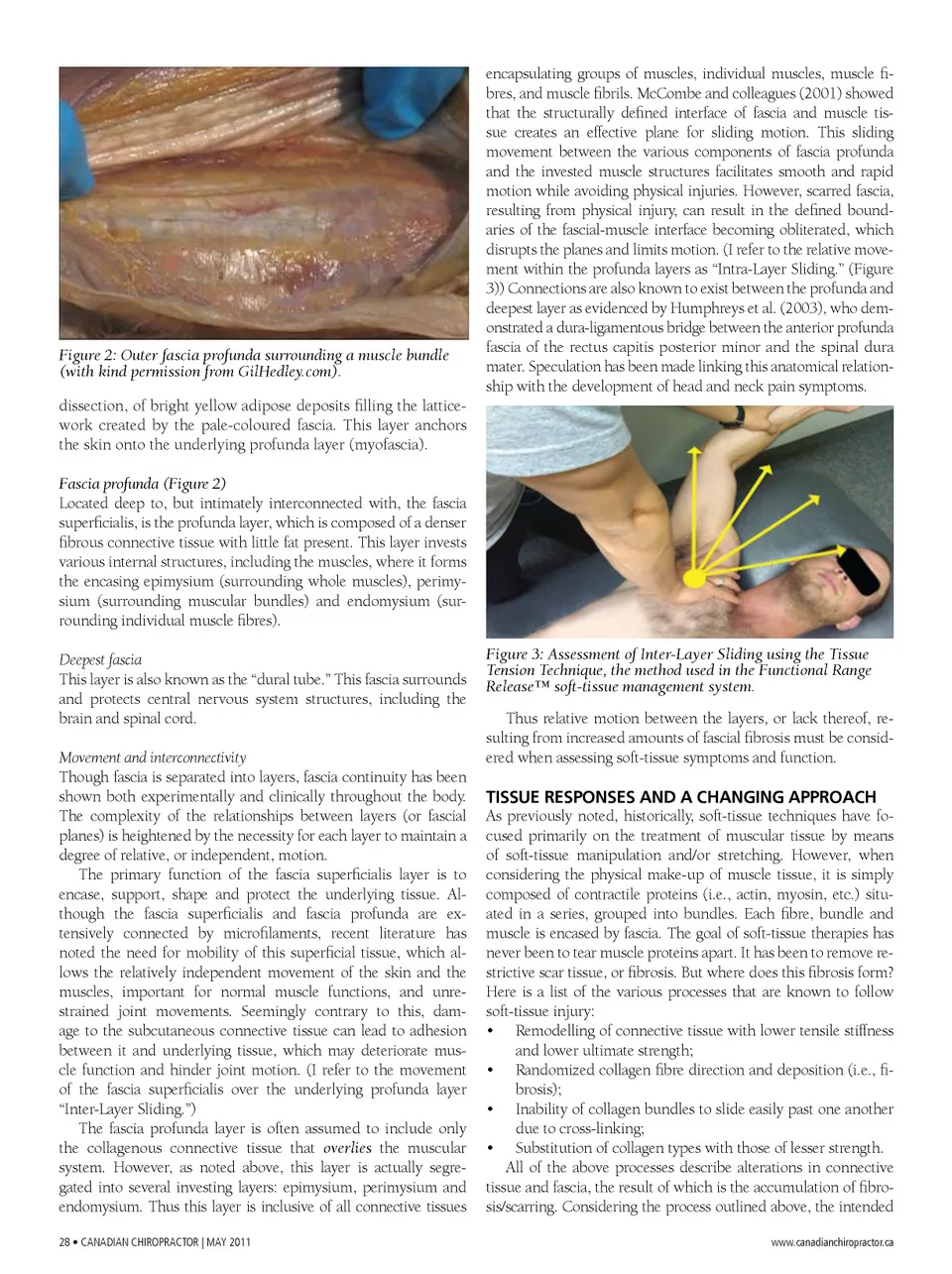
Figure 2: Outer fascia profunda surrounding a muscle bundle (with kind permission from GilHedley.com). dissection, of bright yellow adipose deposits filling the lattice-work created by the pale-coloured fascia. This layer anchors the skin onto the underlying profunda layer (myofascia). Fascia profunda (Figure 2) Located deep to, but intimately interconnected with, the fascia superficialis, is the profunda layer, which is composed of a denser fibrous connective tissue with little fat present. This layer invests various internal structures, including the muscles, where it forms the encasing epimysium (surrounding whole muscles), perimy-sium (surrounding muscular bundles) and endomysium (sur-rounding individual muscle fibres). Deepest fascia This layer is also known as the “dural tube.” This fascia surrounds and protects central nervous system structures, including the brain and spinal cord. Movement and interconnectivity Though fascia is separated into layers, fascia continuity has been shown both experimentally and clinically throughout the body. The complexity of the relationships between layers (or fascial planes) is heightened by the necessity for each layer to maintain a degree of relative, or independent, motion. The primary function of the fascia superficialis layer is to encase, support, shape and protect the underlying tissue. Al-though the fascia superficialis and fascia profunda are ex-tensively connected by microfilaments, recent literature has noted the need for mobility of this superficial tissue, which al-lows the relatively independent movement of the skin and the muscles, important for normal muscle functions, and unre-strained joint movements. Seemingly contrary to this, dam-age to the subcutaneous connective tissue can lead to adhesion between it and underlying tissue, which may deteriorate mus-cle function and hinder joint motion. (I refer to the movement of the fascia superficialis over the underlying profunda layer “Inter-Layer Sliding.”) The fascia profunda layer is often assumed to include only the collagenous connective tissue that overlies the muscular system. However, as noted above, this layer is actually segre-gated into several investing layers: epimysium, perimysium and endomysium. Thus this layer is inclusive of all connective tissues 28 • CANAdiAN CHiROpRACTOR | MAY 2011 encapsulating groups of muscles, individual muscles, muscle fi-bres, and muscle fibrils. McCombe and colleagues (2001) showed that the structurally defined interface of fascia and muscle tis-sue creates an effective plane for sliding motion. This sliding movement between the various components of fascia profunda and the invested muscle structures facilitates smooth and rapid motion while avoiding physical injuries. However, scarred fascia, resulting from physical injury, can result in the defined bound-aries of the fascial-muscle interface becoming obliterated, which disrupts the planes and limits motion. (I refer to the relative move-ment within the profunda layers as “Intra-Layer Sliding.” (Figure 3)) Connections are also known to exist between the profunda and deepest layer as evidenced by Humphreys et al. (2003), who dem -onstrated a dura-ligamentous bridge between the anterior profunda fascia of the rectus capitis posterior minor and the spinal dura mater. Speculation has been made linking this anatomical relation-ship with the development of head and neck pain symptoms. Figure 3: Assessment of Inter-Layer Sliding using the Tissue Tension Technique, the method used in the Functional Range Release™ soft-tissue management system. Thus relative motion between the layers, or lack thereof, re-sulting from increased amounts of fascial fibrosis must be consid-ered when assessing soft-tissue symptoms and function. TISSUE RESPONSES AND A CHANGING APPROACH As previously noted, historically, soft-tissue techniques have fo-cused primarily on the treatment of muscular tissue by means of soft-tissue manipulation and/or stretching. However, when considering the physical make-up of muscle tissue, it is simply composed of contractile proteins (i.e., actin, myosin, etc.) situ-ated in a series, grouped into bundles. Each fibre, bundle and muscle is encased by fascia. The goal of soft-tissue therapies has never been to tear muscle proteins apart. It has been to remove re-strictive scar tissue, or fibrosis. But where does this fibrosis form? Here is a list of the various processes that are known to follow soft-tissue injury: • Remodelling of connective tissue with lower tensile stiffness and lower ultimate strength; • Randomized collagen fibre direction and deposition (i.e., fi-brosis); • Inability of collagen bundles to slide easily past one another due to cross-linking; • Substitution of collagen types with those of lesser strength. All of the above processes describe alterations in connective tissue and fascia, the result of which is the accumulation of fibro-sis/scarring. Considering the process outlined above, the intended www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor May 2011: Page 28