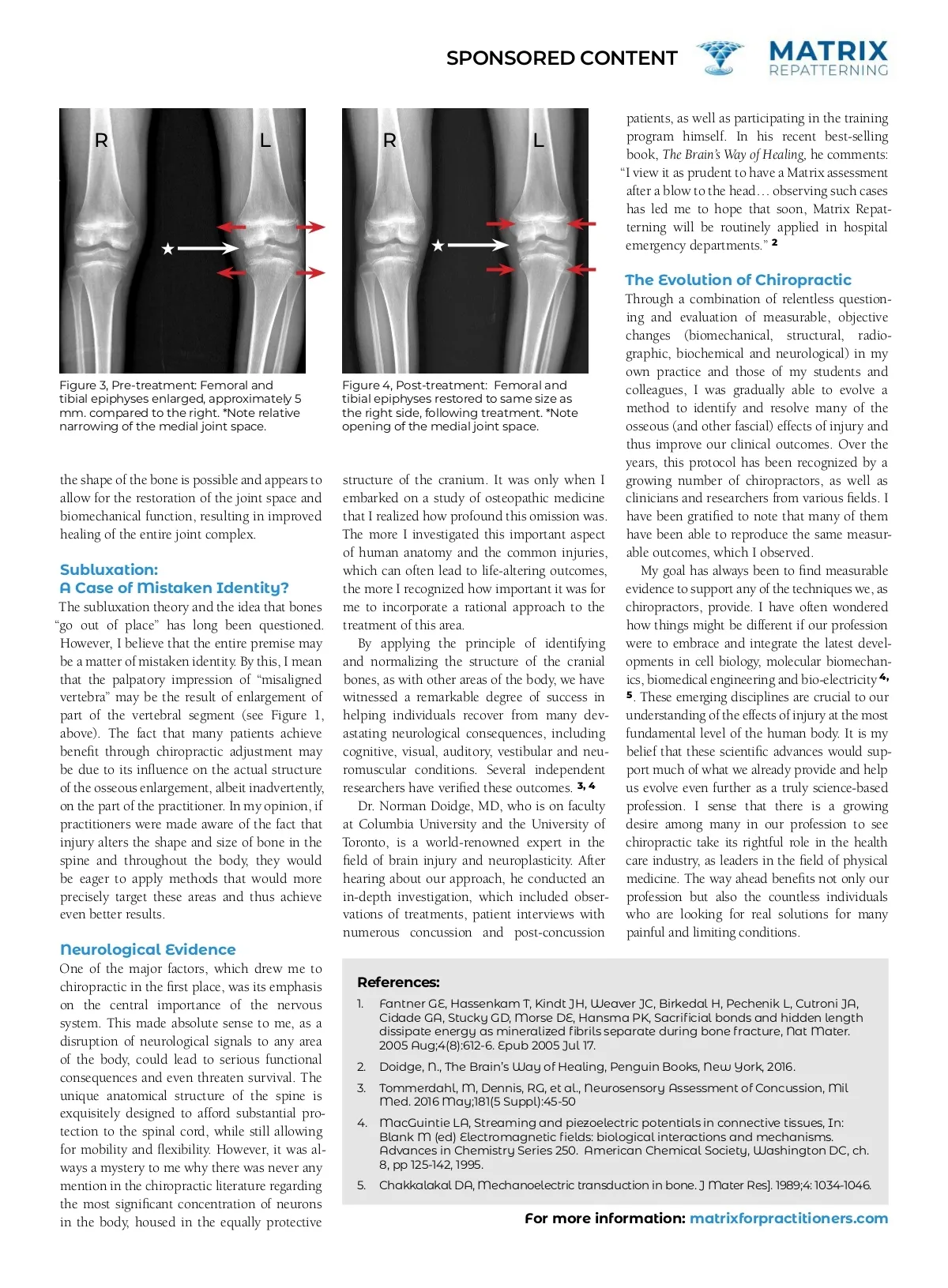
SPONSORED CONTENT Observations in a new light Subluxation: A case of mistaken identity? By Dr. George Roth I recently searched the Internet for scientific evidence to support chiropractic. Unfortu-nately, most of the references emphasized the lack of scientific validation or measur-able outcomes to support the basic tenets of our profession. At best, there are a few studies that demonstrate a modest advantage for chi-ropractic manipulation over some prescription medications for certain conditions, such as back pain. However, the overall impression is that chiropractic science is still relatively un-proven and that chiropractors are only mini-mally accepted as part of the health care team. I have been a chiropractor for over 40 years, but early in my career, I became convinced that I was not achieving the kinds of results prom-ised when I attended school. I also witnessed many of my colleagues becoming disheartened or failing in practice. They had come into this profession with high expectations and a sincere desire to help their fellow humans, but the types of treatments they were taught did not live up to these expectations. Like many of you, I pursued a long search for additional modalities to improve my results, validate my outcomes and give me the confi-dence to be able to find and resolve my patient’s conditions. In this search, I was blessed to meet several researchers and clinicians from other fields (cell biology, biomedical engineering, orthopedic medicine, osteopathy and physical medicine). They were making amazing discov-eries regarding the underlying effects of injury and biomechanical dysfunction at the cellular, bio-electrical and even the molecular level. I recognized that for a system of therapeutics to be valid, it had to be congruent with this emerging science. Startling Observations: Bone Enlarges with Injury! While studying radiology in chiropractic school, I noticed that the size of a structure on one side of the body was often different than its counterpart on the other side. For example, the proximal femoral or humeral head, or the tibial plateau on one side was noticeably larger than the opposite side in the same individual. My professors were unable to shed any light on these findings. As an anatomy lab instructor at the college and from subsequent observations of cadaverous specimens, I was able to confirm these differences. At the time, these facts were filed away, and it was only many years later that these early observations came to be viewed in a new light, based on my clinical research. By carefully examining a better quality skel-etal model, which is cast from a real skeleton, you can verify many of these same discrepan-cies for yourself. Besides the examples of the femur, tibia and humerus mentioned earlier, a close inspection of the spine can be very re-vealing. Note the differences in the size (width, depth and height of the articular processes) at various levels throughout the spine. Figure 1 demonstrates these differences in the size of the articular processes of the atlas. I contend that on palpation, these areas of enlargement may be easily mistaken for a relative rotation or translation of the vertebral segment (see: Sub-luxation: A Case of Mistaken Identity, below). Recent evidence from the University of Cal-ifornia, revealed by the powerful Atomic Force microscope, under the direction of physicist Paul Hansma and his team 1 , has confirmed the presence of certain protein structures within the bone that expand with an injury. These findings are consistent with my clinical obser-vations, which were first made over 40 years ago (see Figure 2). A Testable Hypothesis for a Molecular Origin of Fracture Resistance A Before impact B As an impact begins to separate fibrils C D After the impact is over Figure 2: Microscopic Evidence of Bone Expansion with Injury, Paul Hansma Lab, University of California, Berkeley, 2005. (With permission from the author) Restoration of Bone Size and Joint Healing One of the significant clinical breakthroughs that my colleagues and I were able to ac-complish was that bone size appeared to be restored to normal with treatment. At first, we questioned these results and followed them up with precise measurements using callipers and tape measures. Inter-tester validation appeared to confirm our findings. Several years ago, I treated a 15-year-old Figure 1: Model of C1, cast from a real skeletal specimen. Note the enlargement of the right articular process and the spinal canal, which measured 2 mm. larger in every dimension. male hockey player, who had been suffering from knee pain for several months, which prevented him from playing. The injury also caused considerable pain during normal daily activities, such as climbing stairs, which he was only able to accomplish in a slow, hob-bling manner. Fortunately for me, orthopedic surgeons were monitoring the size of the bones at the knee with a high degree of precision, due to an underlying genetic condition. As a result, they took consistent measurements to within one-hundredth of a millimetre. They were all surprised when the femoral condyle and the tibial plateau of the left knee, which had been approximately 5 mm larger than its counterpart on the right, had suddenly shrunk by that amount after only a few treatments (see Figure 3 and 4). Subsequently, the young man’s parents noted that he was once again “flying up” the stairs with absolutely no pain. This case verified my contention that normalization of
Chiropractic + Naturopathic Doctor December 2019: Page 18