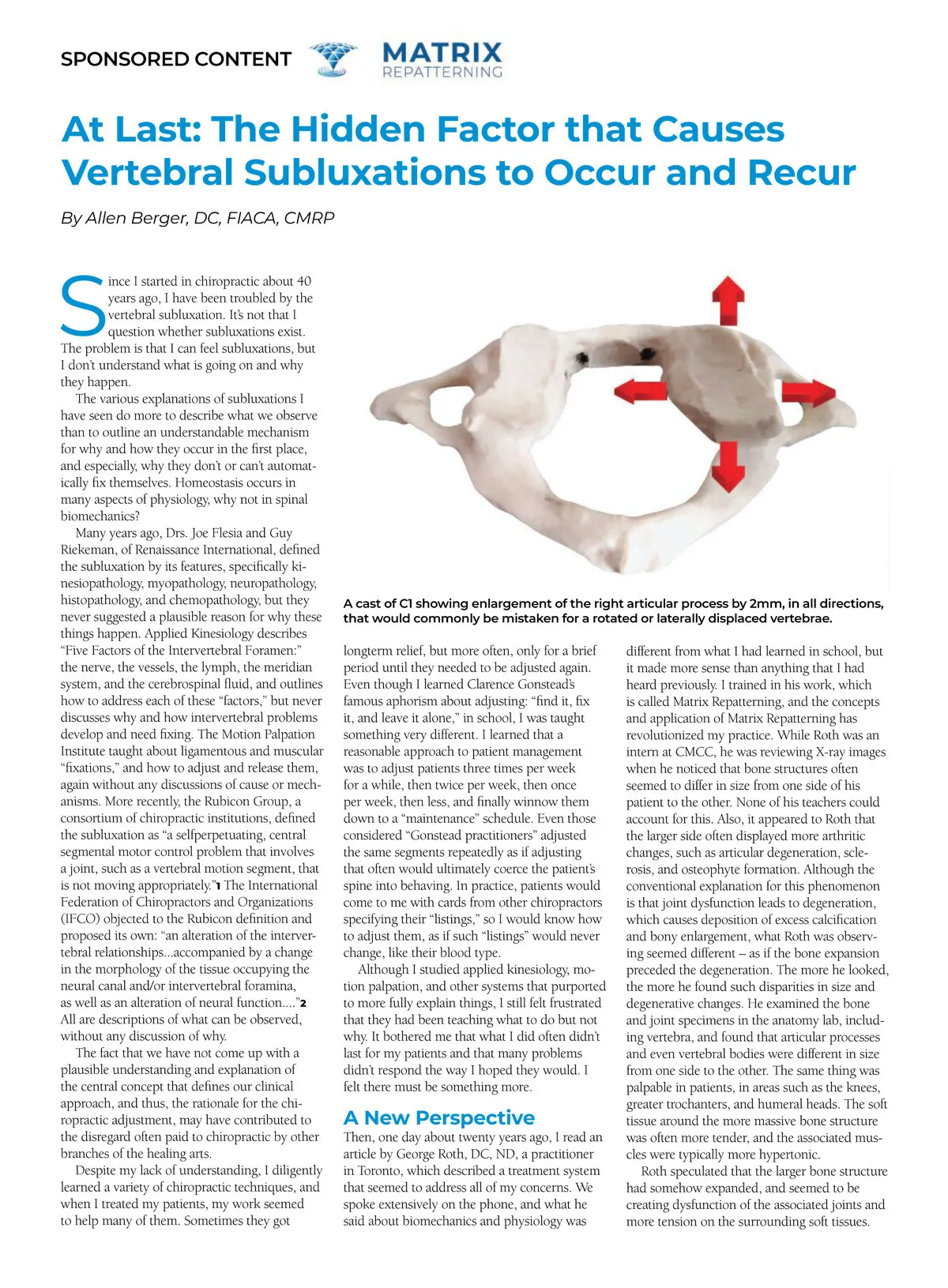
SPONSORED CONTENT At Last: The Hidden Factor that Causes Vertebral Subluxations to Occur and Recur By Allen Berger, DC, FIACA, CMRP S ince I started in chiropractic about 40 years ago, I have been troubled by the vertebral subluxation. It’s not that I question whether subluxations exist. The problem is that I can feel subluxations, but I don’t understand what is going on and why they happen. The various explanations of subluxations I have seen do more to describe what we observe than to outline an understandable mechanism for why and how they occur in the first place, and especially, why they don’t or can’t automat-ically fix themselves. Homeostasis occurs in many aspects of physiology, why not in spinal biomechanics? Many years ago, Drs. Joe Flesia and Guy Riekeman, of Renaissance International, defined the subluxation by its features, specifically ki-nesiopathology, myopathology, neuropathology, histopathology, and chemopathology, but they never suggested a plausible reason for why these things happen. Applied Kinesiology describes “Five Factors of the Intervertebral Foramen:” the nerve, the vessels, the lymph, the meridian system, and the cerebrospinal fluid, and outlines how to address each of these “factors,” but never discusses why and how intervertebral problems develop and need fixing. The Motion Palpation Institute taught about ligamentous and muscular “fixations,” and how to adjust and release them, again without any discussions of cause or mech-anisms. More recently, the Rubicon Group, a consortium of chiropractic institutions, defined the subluxation as “a selfperpetuating, central segmental motor control problem that involves a joint, such as a vertebral motion segment, that is not moving appropriately.” 1 The International Federation of Chiropractors and Organizations (IFCO) objected to the Rubicon definition and proposed its own: “an alteration of the interver-tebral relationships...accompanied by a change in the morphology of the tissue occupying the neural canal and/or intervertebral foramina, as well as an alteration of neural function....” 2 All are descriptions of what can be observed, without any discussion of why. The fact that we have not come up with a plausible understanding and explanation of the central concept that defines our clinical approach, and thus, the rationale for the chi-ropractic adjustment, may have contributed to the disregard often paid to chiropractic by other branches of the healing arts. Despite my lack of understanding, I diligently learned a variety of chiropractic techniques, and when I treated my patients, my work seemed to help many of them. Sometimes they got A cast of C1 showing enlargement of the right articular process by 2mm, in all directions, that would commonly be mistaken for a rotated or laterally displaced vertebrae. longterm relief, but more often, only for a brief period until they needed to be adjusted again. Even though I learned Clarence Gonstead’s famous aphorism about adjusting: “find it, fix it, and leave it alone,” in school, I was taught something very different. I learned that a reasonable approach to patient management was to adjust patients three times per week for a while, then twice per week, then once per week, then less, and finally winnow them down to a “maintenance” schedule. Even those considered “Gonstead practitioners” adjusted the same segments repeatedly as if adjusting that often would ultimately coerce the patient’s spine into behaving. In practice, patients would come to me with cards from other chiropractors specifying their “listings,” so I would know how to adjust them, as if such “listings” would never change, like their blood type. Although I studied applied kinesiology, mo-tion palpation, and other systems that purported to more fully explain things, I still felt frustrated that they had been teaching what to do but not why. It bothered me that what I did often didn’t last for my patients and that many problems didn’t respond the way I hoped they would. I felt there must be something more. A New Perspective Then, one day about twenty years ago, I read an article by George Roth, DC, ND, a practitioner in Toronto, which described a treatment system that seemed to address all of my concerns. We spoke extensively on the phone, and what he said about biomechanics and physiology was different from what I had learned in school, but it made more sense than anything that I had heard previously. I trained in his work, which is called Matrix Repatterning, and the concepts and application of Matrix Repatterning has revolutionized my practice. While Roth was an intern at CMCC, he was reviewing X-ray images when he noticed that bone structures often seemed to differ in size from one side of his patient to the other. None of his teachers could account for this. Also, it appeared to Roth that the larger side often displayed more arthritic changes, such as articular degeneration, scle-rosis, and osteophyte formation. Although the conventional explanation for this phenomenon is that joint dysfunction leads to degeneration, which causes deposition of excess calcification and bony enlargement, what Roth was observ-ing seemed different – as if the bone expansion preceded the degeneration. The more he looked, the more he found such disparities in size and degenerative changes. He examined the bone and joint specimens in the anatomy lab, includ-ing vertebra, and found that articular processes and even vertebral bodies were different in size from one side to the other. The same thing was palpable in patients, in areas such as the knees, greater trochanters, and humeral heads. The soft tissue around the more massive bone structure was often more tender, and the associated mus-cles were typically more hypertonic. Roth speculated that the larger bone structure had somehow expanded, and seemed to be creating dysfunction of the associated joints and more tension on the surrounding soft tissues.
Chiropractic + Naturopathic Doctor JulyAugust 2019: Page 20