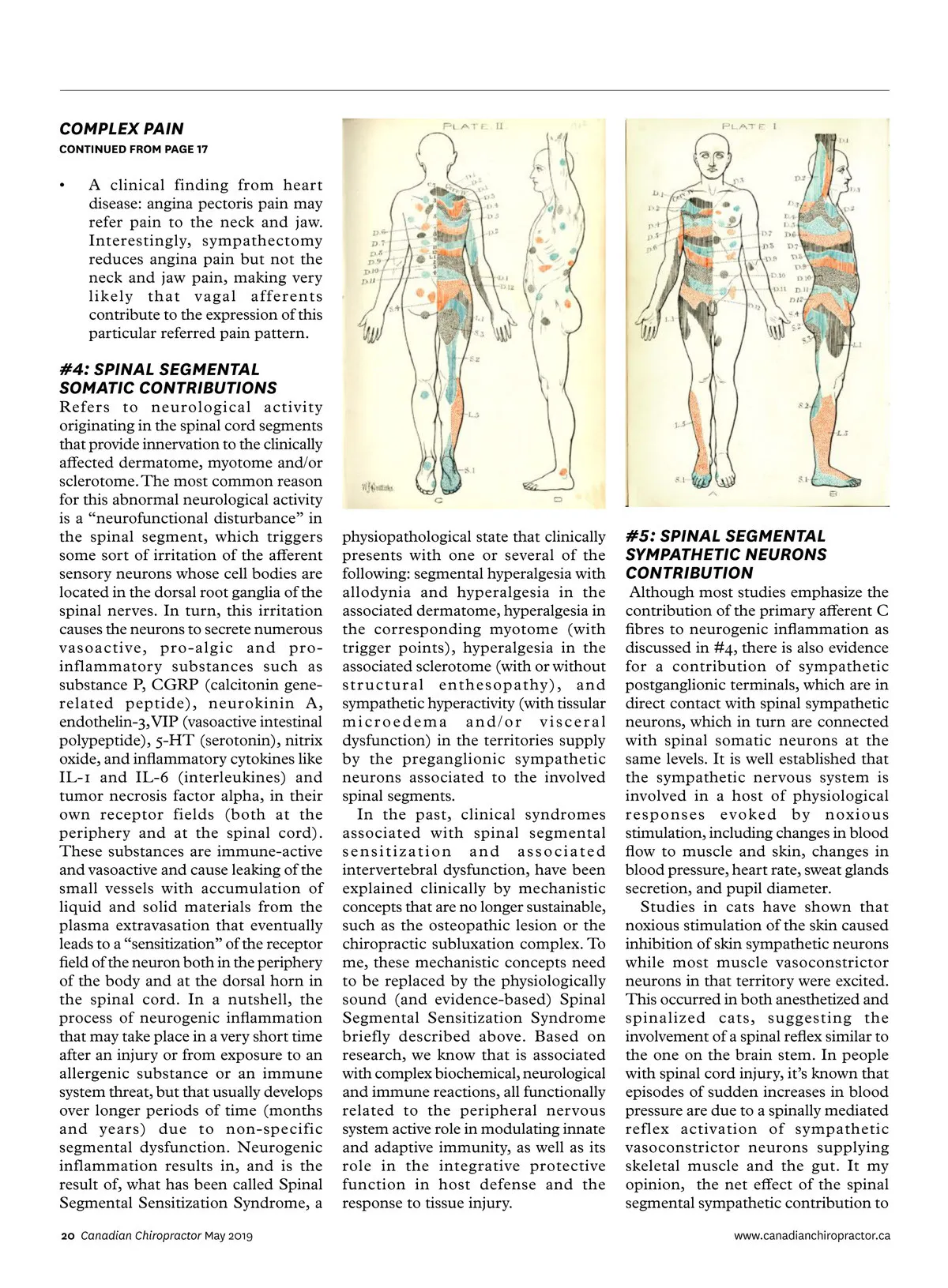
COMPLEX PAIN CONTINUED FROM PAGE 17 • A clinical finding from heart disease: angina pectoris pain may refer pain to the neck and jaw. Interestingly, sympathectomy reduces angina pain but not the neck and jaw pain, making very likely that vagal afferents contribute to the expression of this particular referred pain pattern. #4: SPINAL SEGMENTAL SOMATIC CONTRIBUTIONS Refers to neurological activity originating in the spinal cord segments that provide innervation to the clinically affected dermatome, myotome and/or sclerotome. The most common reason for this abnormal neurological activity is a “neurofunctional disturbance” in the spinal segment, which triggers some sort of irritation of the afferent sensory neurons whose cell bodies are located in the dorsal root ganglia of the spinal nerves. In turn, this irritation causes the neurons to secrete numerous vasoactive, pro-algic and pro-inflammatory substances such as substance P, CGRP (calcitonin gene-related peptide), neurokinin A, endothelin-3, VIP (vasoactive intestinal polypeptide), 5-HT (serotonin), nitrix oxide, and inflammatory cytokines like IL-1 and IL-6 (interleukines) and tumor necrosis factor alpha, in their own receptor fields (both at the periphery and at the spinal cord). These substances are immune-active and vasoactive and cause leaking of the small vessels with accumulation of liquid and solid materials from the plasma extravasation that eventually leads to a “sensitization” of the receptor field of the neuron both in the periphery of the body and at the dorsal horn in the spinal cord. In a nutshell, the process of neurogenic inflammation that may take place in a very short time after an injury or from exposure to an allergenic substance or an immune system threat, but that usually develops over longer periods of time (months and years) due to non-specific segmental dysfunction. Neurogenic inflammation results in, and is the result of, what has been called Spinal Segmental Sensitization Syndrome, a 20 Canadian Chiropractor May 2019 physiopathological state that clinically presents with one or several of the following: segmental hyperalgesia with allodynia and hyperalgesia in the associated dermatome, hyperalgesia in the corresponding myotome (with trigger points), hyperalgesia in the associated sclerotome (with or without structural enthesopathy), and sympathetic hyperactivity (with tissular microedema and/or visceral dysfunction) in the territories supply by the preganglionic sympathetic neurons associated to the involved spinal segments. In the past, clinical syndromes associated with spinal segmental sensitization and associated intervertebral dysfunction, have been explained clinically by mechanistic concepts that are no longer sustainable, such as the osteopathic lesion or the chiropractic subluxation complex. To me, these mechanistic concepts need to be replaced by the physiologically sound (and evidence-based) Spinal Segmental Sensitization Syndrome briefly described above. Based on research, we know that is associated with complex biochemical, neurological and immune reactions, all functionally related to the peripheral nervous system active role in modulating innate and adaptive immunity, as well as its role in the integrative protective function in host defense and the response to tissue injury. #5: SPINAL SEGMENTAL SYMPATHETIC NEURONS CONTRIBUTION Although most studies emphasize the contribution of the primary afferent C fibres to neurogenic inflammation as discussed in #4, there is also evidence for a contribution of sympathetic postganglionic terminals, which are in direct contact with spinal sympathetic neurons, which in turn are connected with spinal somatic neurons at the same levels. It is well established that the sympathetic nervous system is involved in a host of physiological responses evoked by noxious stimulation, including changes in blood flow to muscle and skin, changes in blood pressure, heart rate, sweat glands secretion, and pupil diameter. Studies in cats have shown that noxious stimulation of the skin caused inhibition of skin sympathetic neurons while most muscle vasoconstrictor neurons in that territory were excited. This occurred in both anesthetized and spinalized cats, suggesting the involvement of a spinal reflex similar to the one on the brain stem. In people with spinal cord injury, it’s known that episodes of sudden increases in blood pressure are due to a spinally mediated reflex activation of sympathetic vasoconstrictor neurons supplying skeletal muscle and the gut. It my opinion, the net effect of the spinal segmental sympathetic contribution to www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor May 2019: Page 20