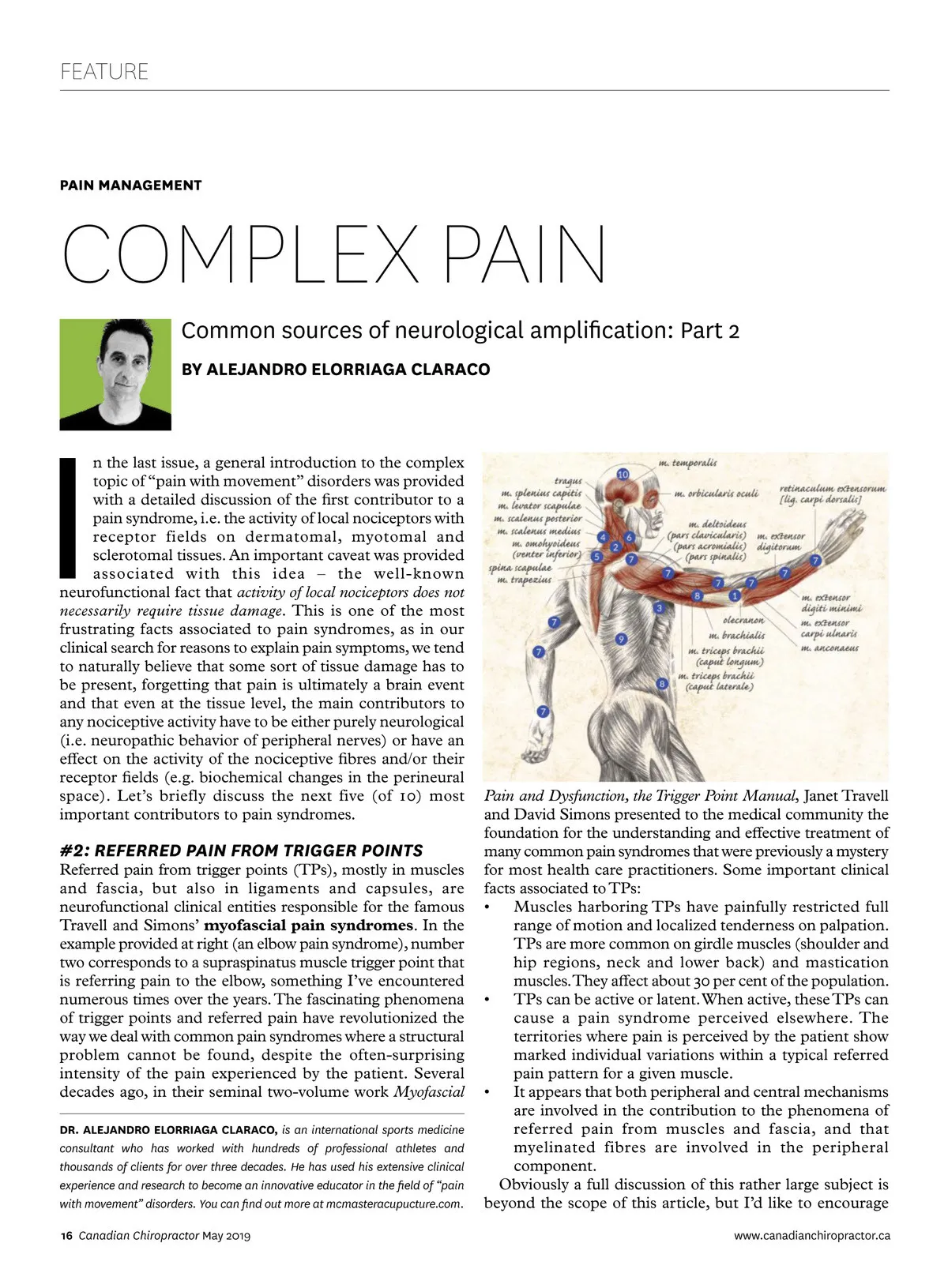
FEATURE PAIN MANAGEMENT COMPLEX PAIN Common sources of neurological amplification: Part 2 BY ALEJANDRO ELORRIAGA CLARACO I n the last issue, a general introduction to the complex topic of “pain with movement” disorders was provided with a detailed discussion of the first contributor to a pain syndrome, i.e. the activity of local nociceptors with receptor fields on dermatomal, myotomal and sclerotomal tissues. An important caveat was provided associated with this idea – the well-known neurofunctional fact that activity of local nociceptors does not necessarily require tissue damage. This is one of the most frustrating facts associated to pain syndromes, as in our clinical search for reasons to explain pain symptoms, we tend to naturally believe that some sort of tissue damage has to be present, forgetting that pain is ultimately a brain event and that even at the tissue level, the main contributors to any nociceptive activity have to be either purely neurological (i.e. neuropathic behavior of peripheral nerves) or have an effect on the activity of the nociceptive fibres and/or their receptor fields (e.g. biochemical changes in the perineural space). Let’s briefly discuss the next five (of 10) most important contributors to pain syndromes. #2: REFERRED PAIN FROM TRIGGER POINTS Referred pain from trigger points (TPs), mostly in muscles and fascia, but also in ligaments and capsules, are neurofunctional clinical entities responsible for the famous Travell and Simons’ myofascial pain syndromes . In the example provided at right (an elbow pain syndrome), number two corresponds to a supraspinatus muscle trigger point that is referring pain to the elbow, something I’ve encountered numerous times over the years. The fascinating phenomena of trigger points and referred pain have revolutionized the way we deal with common pain syndromes where a structural problem cannot be found, despite the often-surprising intensity of the pain experienced by the patient. Several decades ago, in their seminal two-volume work Myofascial DR. ALEJANDRO ELORRIAGA CLARACO, is an international sports medicine consultant who has worked with hundreds of professional athletes and thousands of clients for over three decades. He has used his extensive clinical experience and research to become an innovative educator in the field of “pain with movement” disorders. You can find out more at mcmasteracupucture.com. 16 Canadian Chiropractor May 2019 Pain and Dysfunction, the Trigger Point Manual , Janet Travell and David Simons presented to the medical community the foundation for the understanding and effective treatment of many common pain syndromes that were previously a mystery for most health care practitioners. Some important clinical facts associated to TPs: • Muscles harboring TPs have painfully restricted full range of motion and localized tenderness on palpation. TPs are more common on girdle muscles (shoulder and hip regions, neck and lower back) and mastication muscles. They affect about 30 per cent of the population. • TPs can be active or latent. When active, these TPs can cause a pain syndrome perceived elsewhere. The territories where pain is perceived by the patient show marked individual variations within a typical referred pain pattern for a given muscle. • It appears that both peripheral and central mechanisms are involved in the contribution to the phenomena of referred pain from muscles and fascia, and that myelinated fibres are involved in the peripheral component. Obviously a full discussion of this rather large subject is beyond the scope of this article, but I’d like to encourage www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor May 2019: Page 16