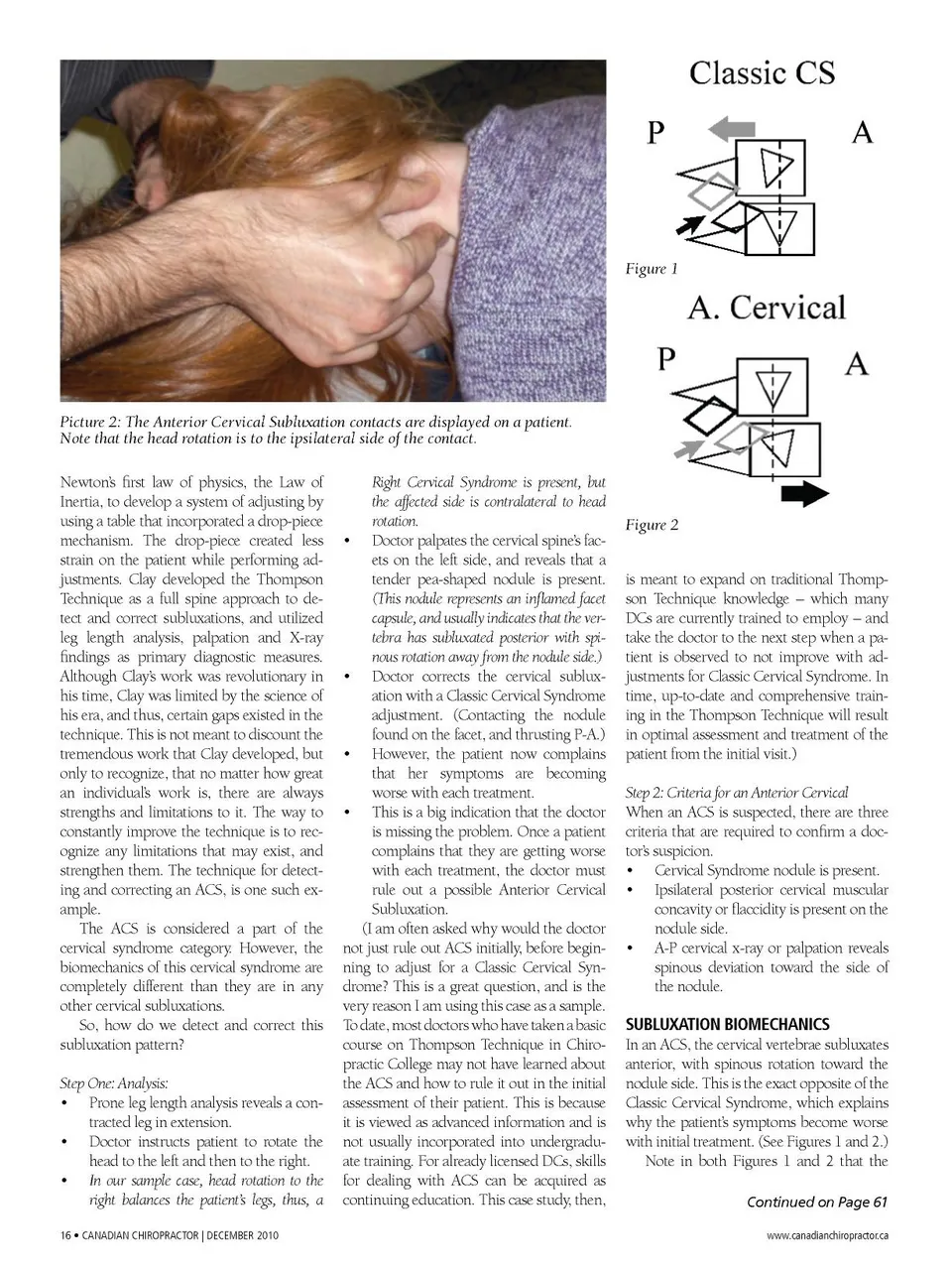
Figure 1 Picture 2: The Anterior Cervical Subluxation contacts are displayed on a patient. Note that the head rotation is to the ipsilateral side of the contact. Newton’s first law of physics, the Law of Inertia, to develop a system of adjusting by using a table that incorporated a drop-piece mechanism. The drop-piece created less strain on the patient while performing ad-justments. Clay developed the Thompson Technique as a full spine approach to de-tect and correct subluxations, and utilized leg length analysis, palpation and X-ray findings as primary diagnostic measures. Although Clay’s work was revolutionary in his time, Clay was limited by the science of his era, and thus, certain gaps existed in the technique. This is not meant to discount the tremendous work that Clay developed, but only to recognize, that no matter how great an individual’s work is, there are always strengths and limitations to it. The way to constantly improve the technique is to rec-ognize any limitations that may exist, and strengthen them. The technique for detect-ing and correcting an ACS, is one such ex-ample. The ACS is considered a part of the cervical syndrome category. However, the biomechanics of this cervical syndrome are completely different than they are in any other cervical subluxations. So, how do we detect and correct this subluxation pattern? Step One: Analysis: • Prone leg length analysis reveals a con-tracted leg in extension. • Doctor instructs patient to rotate the head to the left and then to the right. • In our sample case, head rotation to the right balances the patient’s legs, thus, a 16 • CaNaDIaN CHIROPRaCTOR | DECEMBER 2010 Right Cervical Syndrome is present, but the affected side is contralateral to head rotation. • Doctor palpates the cervical spine’s fac-ets on the left side, and reveals that a tender pea-shaped nodule is present. (This nodule represents an inflamed facet capsule, and usually indicates that the ver-tebra has subluxated posterior with spi-nous rotation away from the nodule side.) • Doctor corrects the cervical sublux-ation with a Classic Cervical Syndrome adjustment. (Contacting the nodule found on the facet, and thrusting P-A.) • However, the patient now complains that her symptoms are becoming worse with each treatment. • This is a big indication that the doctor is missing the problem. Once a patient complains that they are getting worse with each treatment, the doctor must rule out a possible Anterior Cervical Subluxation. (I am often asked why would the doctor not just rule out ACS initially, before begin-ning to adjust for a Classic Cervical Syn-drome? This is a great question, and is the very reason I am using this case as a sample. To date, most doctors who have taken a basic course on Thompson Technique in Chiro-practic College may not have learned about the ACS and how to rule it out in the initial assessment of their patient. This is because it is viewed as advanced information and is not usually incorporated into undergradu-ate training. For already licensed DCs, skills for dealing with ACS can be acquired as continuing education. This case study, then, Figure 2 is meant to expand on traditional Thomp-son Technique knowledge – which many DCs are currently trained to employ – and take the doctor to the next step when a pa-tient is observed to not improve with ad-justments for Classic Cervical Syndrome. In time, up-to-date and comprehensive train-ing in the Thompson Technique will result in optimal assessment and treatment of the patient from the initial visit.) Step 2: Criteria for an Anterior Cervical When an ACS is suspected, there are three criteria that are required to confirm a doc-tor’s suspicion. • Cervical Syndrome nodule is present. • Ipsilateral posterior cervical muscular concavity or flaccidity is present on the nodule side. • A-P cervical x-ray or palpation reveals spinous deviation toward the side of the nodule. SUBLUXATION BIOMECHANICS In an ACS, the cervical vertebrae subluxates anterior, with spinous rotation toward the nodule side. This is the exact opposite of the Classic Cervical Syndrome, which explains why the patient’s symptoms become worse with initial treatment. (See Figures 1 and 2.) Note in both Figures 1 and 2 that the Continued on Page 61 www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor December 2010: Page 16