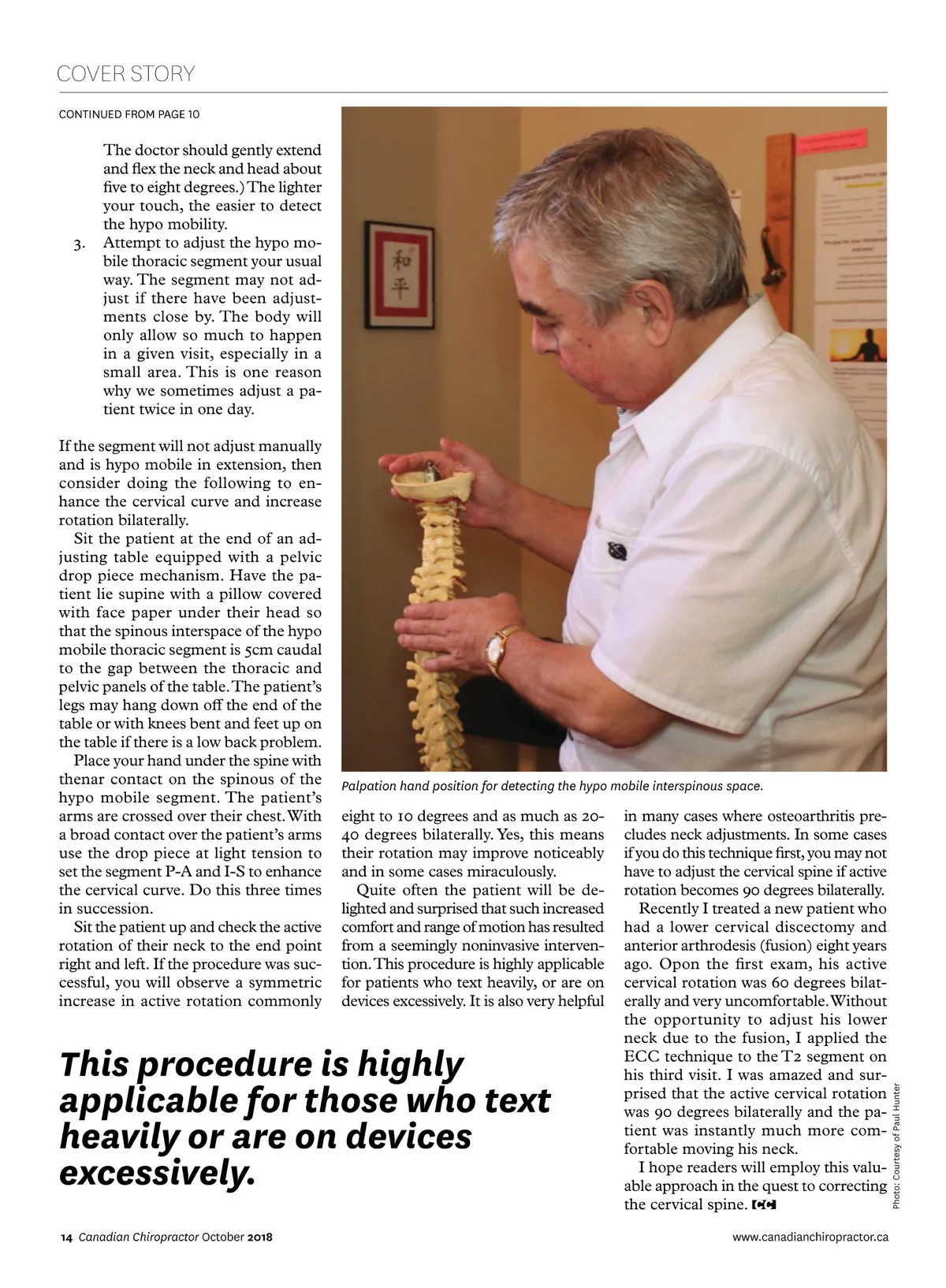
COVER STORY CONTINUED FROM PAGE 10 3. The doctor should gently extend and flex the neck and head about five to eight degrees.) The lighter your touch, the easier to detect the hypo mobility. Attempt to adjust the hypo mo-bile thoracic segment your usual way. The segment may not ad-just if there have been adjust-ments close by. The body will only allow so much to happen in a given visit, especially in a small area. This is one reason why we sometimes adjust a pa-tient twice in one day. If the segment will not adjust manually and is hypo mobile in extension, then consider doing the following to en-hance the cervical curve and increase rotation bilaterally. Sit the patient at the end of an ad-justing table equipped with a pelvic drop piece mechanism. Have the pa-tient lie supine with a pillow covered with face paper under their head so that the spinous interspace of the hypo mobile thoracic segment is 5cm caudal to the gap between the thoracic and pelvic panels of the table. The patient’s legs may hang down off the end of the table or with knees bent and feet up on the table if there is a low back problem. Place your hand under the spine with thenar contact on the spinous of the hypo mobile segment. The patient’s arms are crossed over their chest. With a broad contact over the patient’s arms use the drop piece at light tension to set the segment P-A and I-S to enhance the cervical curve. Do this three times in succession. Sit the patient up and check the active rotation of their neck to the end point right and left. If the procedure was suc-cessful, you will observe a symmetric increase in active rotation commonly Palpation hand position for detecting the hypo mobile interspinous space. eight to 10 degrees and as much as 20-40 degrees bilaterally. Yes, this means their rotation may improve noticeably and in some cases miraculously. Quite often the patient will be de-lighted and surprised that such increased comfort and range of motion has resulted from a seemingly noninvasive interven-tion. This procedure is highly applicable for patients who text heavily, or are on devices excessively. It is also very helpful 14 Canadian Chiropractor October 2018 www.canadianchiropractor.ca Photo: Courtesy of Paul Hunter This procedure is highly applicable for those who text heavily or are on devices excessively. in many cases where osteoarthritis pre-cludes neck adjustments. In some cases if you do this technique first, you may not have to adjust the cervical spine if active rotation becomes 90 degrees bilaterally. Recently I treated a new patient who had a lower cervical discectomy and anterior arthrodesis (fusion) eight years ago. Opon the first exam, his active cervical rotation was 60 degrees bilat-erally and very uncomfortable. Without the opportunity to adjust his lower neck due to the fusion, I applied the ECC technique to the T2 segment on his third visit. I was amazed and sur-prised that the active cervical rotation was 90 degrees bilaterally and the pa-tient was instantly much more com-fortable moving his neck. I hope readers will employ this valu-able approach in the quest to correcting the cervical spine.
Chiropractic + Naturopathic Doctor October 2018: Page 14