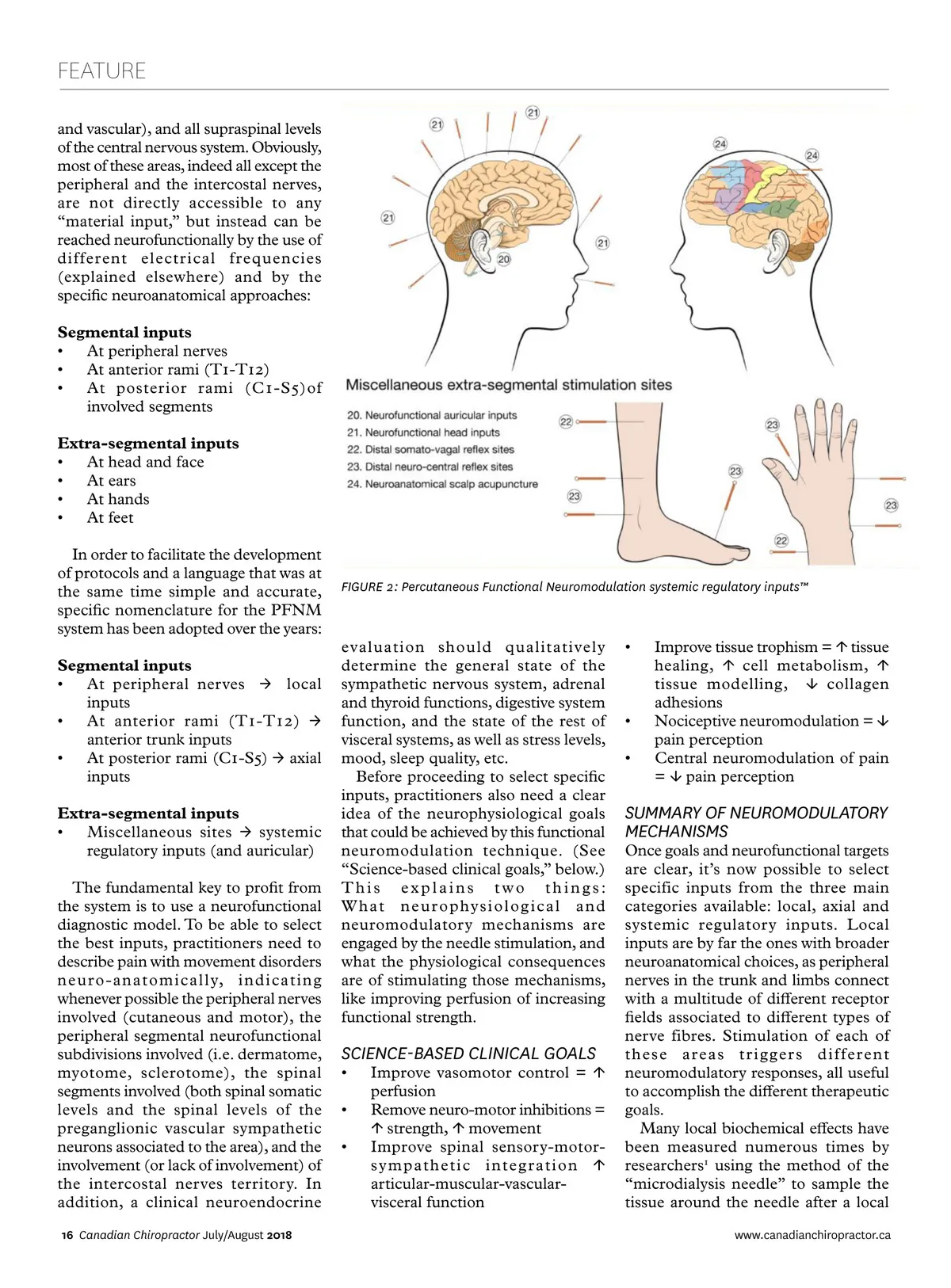
FEATURE and vascular), and all supraspinal levels of the central nervous system. Obviously, most of these areas, indeed all except the peripheral and the intercostal nerves, are not directly accessible to any “material input,” but instead can be reached neurofunctionally by the use of different electrical frequencies (explained elsewhere) and by the specific neuroanatomical approaches: Segmental inputs • At peripheral nerves • At anterior rami (T1-T12) • At posterior rami (C1-S5)of involved segments Extra-segmental inputs • At head and face • At ears • At hands • At feet In order to facilitate the development of protocols and a language that was at the same time simple and accurate, specific nomenclature for the PFNM system has been adopted over the years: Segmental inputs • At peripheral nerves → local inputs • At anterior rami (T1-T12) → anterior trunk inputs • At posterior rami (C1-S5) → axial inputs Extra-segmental inputs • Miscellaneous sites → systemic regulatory inputs (and auricular) The fundamental key to profit from the system is to use a neurofunctional diagnostic model. To be able to select the best inputs, practitioners need to describe pain with movement disorders neuro-anatomically, indicating whenever possible the peripheral nerves involved (cutaneous and motor), the peripheral segmental neurofunctional subdivisions involved (i.e. dermatome, myotome, sclerotome), the spinal segments involved (both spinal somatic levels and the spinal levels of the preganglionic vascular sympathetic neurons associated to the area), and the involvement (or lack of involvement) of the intercostal nerves territory. In addition, a clinical neuroendocrine 16 Canadian Chiropractor July/August 2018 FIGURE 2: Percutaneous Functional Neuromodulation systemic regulatory inputs™ evaluation should qualitatively determine the general state of the sympathetic nervous system, adrenal and thyroid functions, digestive system function, and the state of the rest of visceral systems, as well as stress levels, mood, sleep quality, etc. Before proceeding to select specific inputs, practitioners also need a clear idea of the neurophysiological goals that could be achieved by this functional neuromodulation technique. (See “Science-based clinical goals,” below.) This explains two things: What neurophysiological and neuromodulatory mechanisms are engaged by the needle stimulation, and what the physiological consequences are of stimulating those mechanisms, like improving perfusion of increasing functional strength. • • • Improve tissue trophism = ↑ tissue healing, ↑ cell metabolism, ↑ tissue modelling, ↓ collagen adhesions Nociceptive neuromodulation = ↓ pain perception Central neuromodulation of pain = ↓ pain perception SUMMARY OF NEUROMODULATORY MECHANISMS SCIENCE-BASED CLINICAL GOALS • • • Improve vasomotor control = ↑ perfusion Remove neuro-motor inhibitions = ↑ strength, ↑ movement Improve spinal sensory-motor-sympathetic integration ↑ articular-muscular-vascular-visceral function Once goals and neurofunctional targets are clear, it’s now possible to select specific inputs from the three main categories available: local, axial and systemic regulatory inputs. Local inputs are by far the ones with broader neuroanatomical choices, as peripheral nerves in the trunk and limbs connect with a multitude of different receptor fields associated to different types of nerve fibres. Stimulation of each of these areas triggers different neuromodulatory responses, all useful to accomplish the different therapeutic goals. Many local biochemical effects have been measured numerous times by researchers 1 using the method of the “microdialysis needle” to sample the tissue around the needle after a local www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor July/August 2018: Page 16