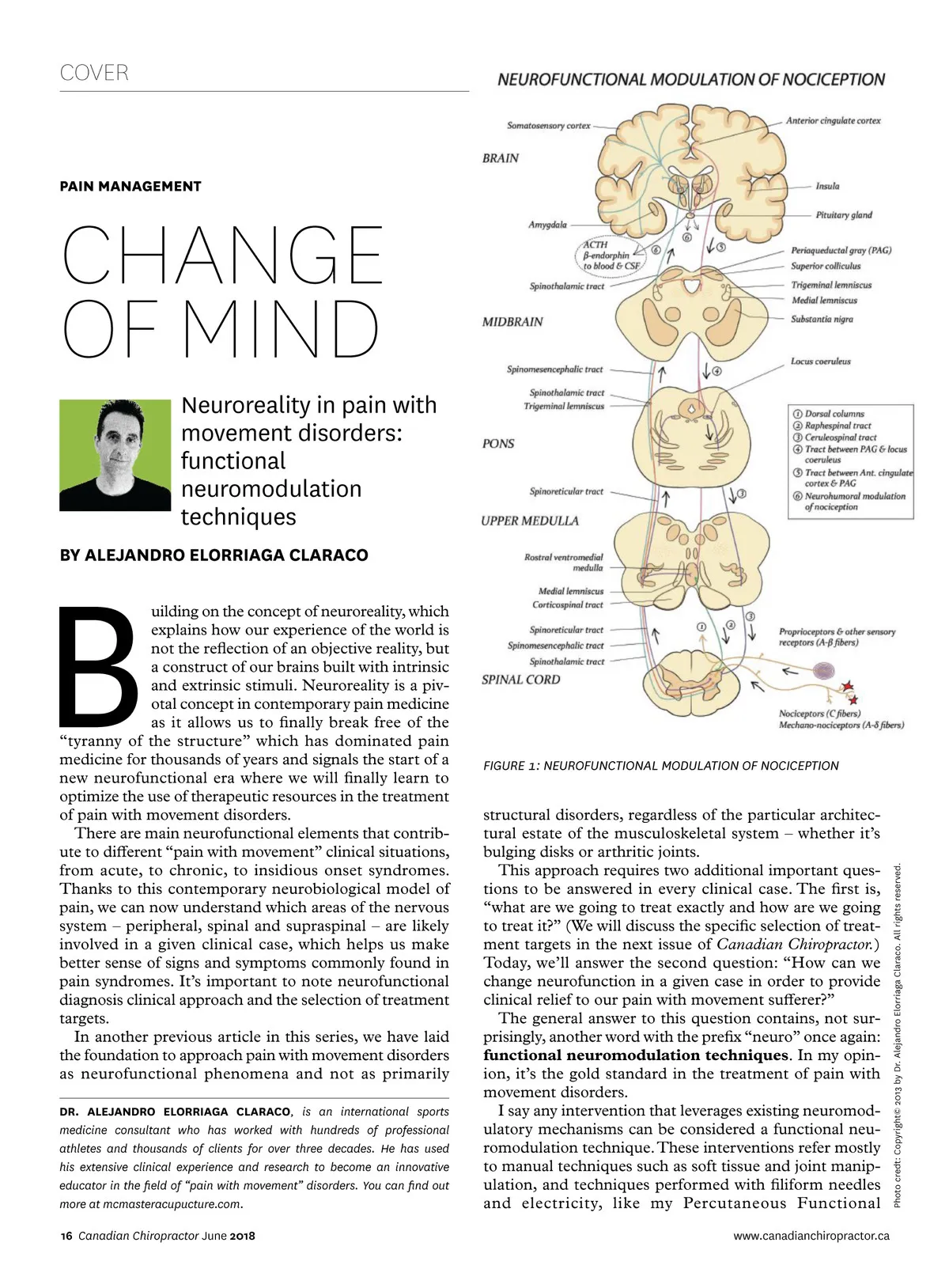
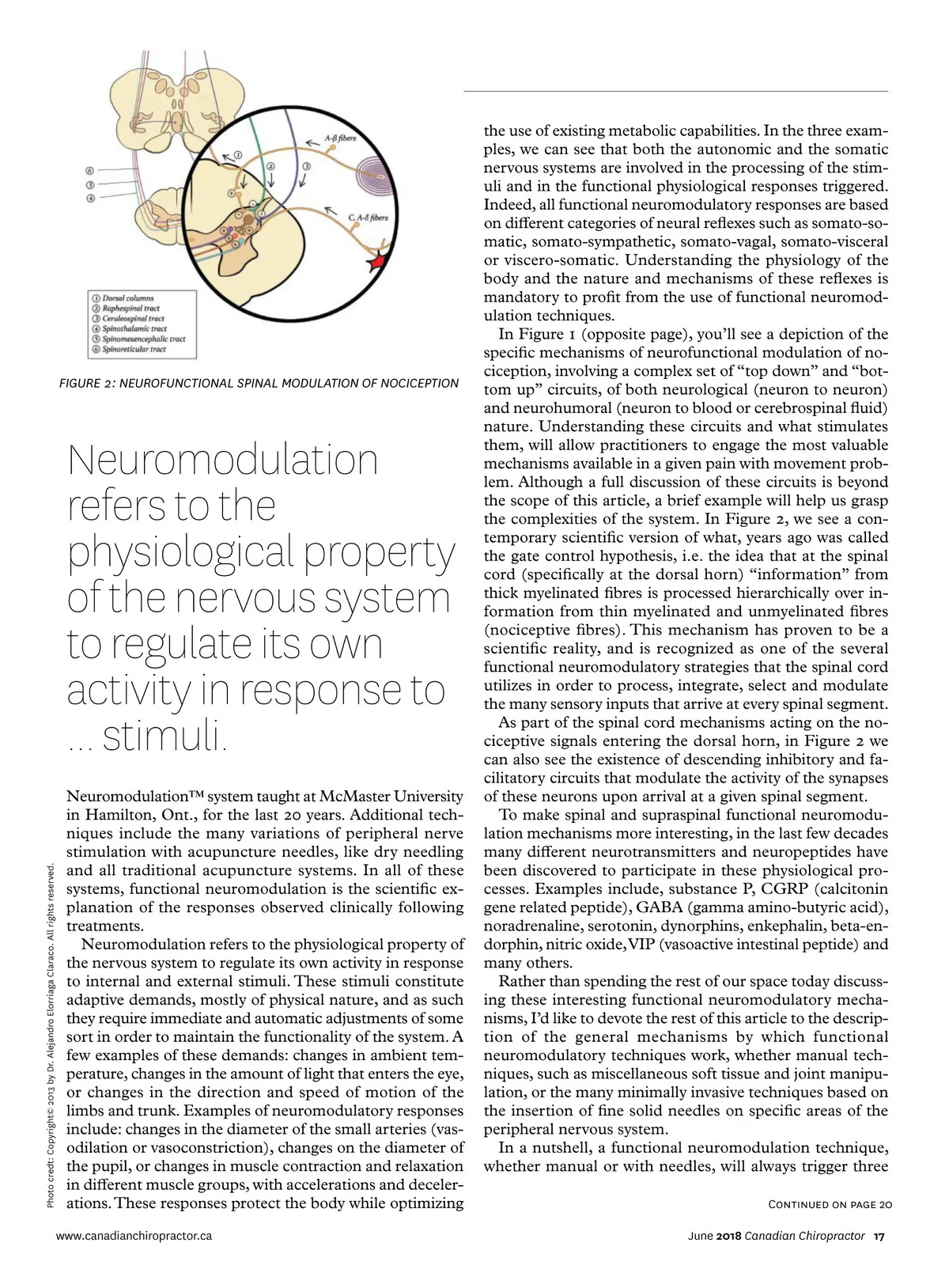
FIGURE 2: NEUROFUNCTIONAL SPINAL MODULATION OF NOCICEPTION Neuromodulation refers to the physiological property of the nervous system to regulate its own activity in response to ... stimuli. Neuromodulation™ system taught at McMaster University in Hamilton, Ont., for the last 20 years. Additional tech-niques include the many variations of peripheral nerve stimulation with acupuncture needles, like dry needling and all traditional acupuncture systems. In all of these systems, functional neuromodulation is the scientific ex-planation of the responses observed clinically following treatments. Neuromodulation refers to the physiological property of the nervous system to regulate its own activity in response to internal and external stimuli. These stimuli constitute adaptive demands, mostly of physical nature, and as such they require immediate and automatic adjustments of some sort in order to maintain the functionality of the system. A few examples of these demands: changes in ambient tem-perature, changes in the amount of light that enters the eye, or changes in the direction and speed of motion of the limbs and trunk. Examples of neuromodulatory responses include: changes in the diameter of the small arteries (vas-odilation or vasoconstriction), changes on the diameter of the pupil, or changes in muscle contraction and relaxation in different muscle groups, with accelerations and deceler-ations. These responses protect the body while optimizing www.canadianchiropractor.ca Photo credt: Copyright© 2013 by Dr. Alejandro Elorriaga Claraco. All rights reserved. the use of existing metabolic capabilities. In the three exam-ples, we can see that both the autonomic and the somatic nervous systems are involved in the processing of the stim-uli and in the functional physiological responses triggered. Indeed, all functional neuromodulatory responses are based on different categories of neural reflexes such as somato-so-matic, somato-sympathetic, somato-vagal, somato-visceral or viscero-somatic. Understanding the physiology of the body and the nature and mechanisms of these reflexes is mandatory to profit from the use of functional neuromod-ulation techniques. In Figure 1 (opposite page), you’ll see a depiction of the specific mechanisms of neurofunctional modulation of no-ciception, involving a complex set of “top down” and “bot-tom up” circuits, of both neurological (neuron to neuron) and neurohumoral (neuron to blood or cerebrospinal fluid) nature. Understanding these circuits and what stimulates them, will allow practitioners to engage the most valuable mechanisms available in a given pain with movement prob-lem. Although a full discussion of these circuits is beyond the scope of this article, a brief example will help us grasp the complexities of the system. In Figure 2, we see a con-temporary scientific version of what, years ago was called the gate control hypothesis, i.e. the idea that at the spinal cord (specifically at the dorsal horn) “information” from thick myelinated fibres is processed hierarchically over in-formation from thin myelinated and unmyelinated fibres (nociceptive fibres). This mechanism has proven to be a scientific reality, and is recognized as one of the several functional neuromodulatory strategies that the spinal cord utilizes in order to process, integrate, select and modulate the many sensory inputs that arrive at every spinal segment. As part of the spinal cord mechanisms acting on the no-ciceptive signals entering the dorsal horn, in Figure 2 we can also see the existence of descending inhibitory and fa-cilitatory circuits that modulate the activity of the synapses of these neurons upon arrival at a given spinal segment. To make spinal and supraspinal functional neuromodu-lation mechanisms more interesting, in the last few decades many different neurotransmitters and neuropeptides have been discovered to participate in these physiological pro-cesses. Examples include, substance P, CGRP (calcitonin gene related peptide), GABA (gamma amino-butyric acid), noradrenaline, serotonin, dynorphins, enkephalin, beta-en-dorphin, nitric oxide, VIP (vasoactive intestinal peptide) and many others. Rather than spending the rest of our space today discuss-ing these interesting functional neuromodulatory mecha-nisms, I’d like to devote the rest of this article to the descrip-tion of the general mechanisms by which functional neuromodulatory techniques work, whether manual tech-niques, such as miscellaneous soft tissue and joint manipu-lation, or the many minimally invasive techniques based on the insertion of fine solid needles on specific areas of the peripheral nervous system. In a nutshell, a functional neuromodulation technique, whether manual or with needles, will always trigger three Continued on page 20 June 2018 Canadian Chiropractor 17
Chiropractic + Naturopathic Doctor June 2018: Page 17