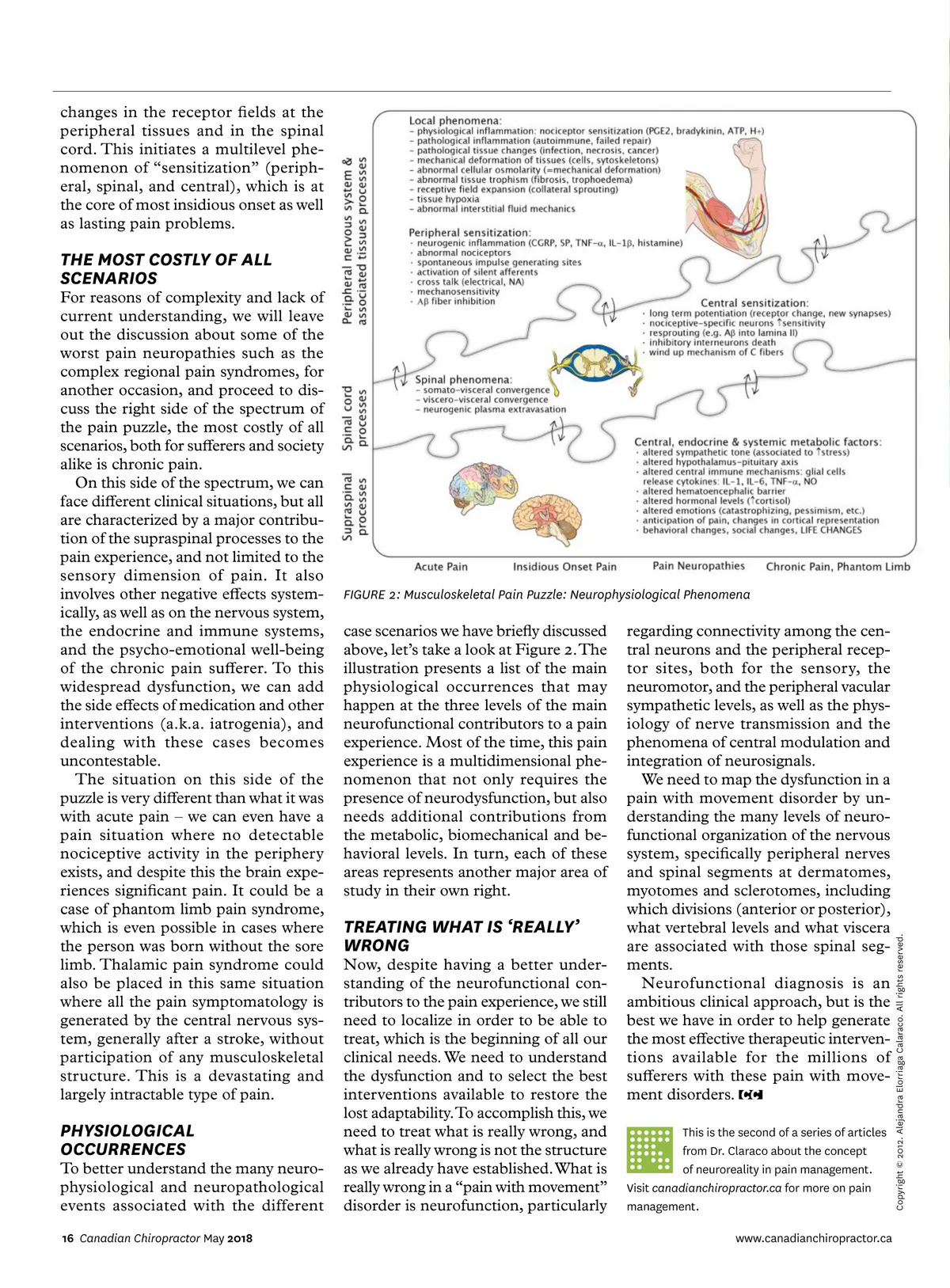
changes in the receptor fields at the peripheral tissues and in the spinal cord. This initiates a multilevel phe-nomenon of “sensitization” (periph-eral, spinal, and central), which is at the core of most insidious onset as well as lasting pain problems. THE MOST COSTLY OF ALL SCENARIOS PHYSIOLOGICAL OCCURRENCES To better understand the many neuro-physiological and neuropathological events associated with the different 16 Canadian Chiropractor May 2018 Now, despite having a better under-standing of the neurofunctional con-tributors to the pain experience, we still need to localize in order to be able to treat, which is the beginning of all our clinical needs. We need to understand the dysfunction and to select the best interventions available to restore the lost adaptability. To accomplish this, we need to treat what is really wrong, and what is really wrong is not the structure as we already have established. What is really wrong in a “pain with movement” disorder is neurofunction, particularly This is the second of a series of articles from Dr. Claraco about the concept of neuroreality in pain management. Visit canadianchiropractor.ca for more on pain management. www.canadianchiropractor.ca Copyright © 2012. Alejandra Elorriaga Calaraco. All rights reserved. For reasons of complexity and lack of current understanding, we will leave out the discussion about some of the worst pain neuropathies such as the complex regional pain syndromes, for another occasion, and proceed to dis-cuss the right side of the spectrum of the pain puzzle, the most costly of all scenarios, both for sufferers and society alike is chronic pain. On this side of the spectrum, we can face different clinical situations, but all are characterized by a major contribu-tion of the supraspinal processes to the pain experience, and not limited to the sensory dimension of pain. It also involves other negative effects system-ically, as well as on the nervous system, the endocrine and immune systems, and the psycho-emotional well-being of the chronic pain sufferer. To this widespread dysfunction, we can add the side effects of medication and other interventions (a.k.a. iatrogenia), and dealing with these cases becomes uncontestable. The situation on this side of the puzzle is very different than what it was with acute pain – we can even have a pain situation where no detectable nociceptive activity in the periphery exists, and despite this the brain expe-riences significant pain. It could be a case of phantom limb pain syndrome, which is even possible in cases where the person was born without the sore limb. Thalamic pain syndrome could also be placed in this same situation where all the pain symptomatology is generated by the central nervous sys-tem, generally after a stroke, without participation of any musculoskeletal structure. This is a devastating and largely intractable type of pain. FIGURE 2: Musculoskeletal Pain Puzzle: Neurophysiological Phenomena case scenarios we have briefly discussed above, let’s take a look at Figure 2. The illustration presents a list of the main physiological occurrences that may happen at the three levels of the main neurofunctional contributors to a pain experience. Most of the time, this pain experience is a multidimensional phe-nomenon that not only requires the presence of neurodysfunction, but also needs additional contributions from the metabolic, biomechanical and be-havioral levels. In turn, each of these areas represents another major area of study in their own right. TREATING WHAT IS ‘REALLY’ WRONG regarding connectivity among the cen-tral neurons and the peripheral recep-tor sites, both for the sensory, the neuromotor, and the peripheral vacular sympathetic levels, as well as the phys-iology of nerve transmission and the phenomena of central modulation and integration of neurosignals. We need to map the dysfunction in a pain with movement disorder by un-derstanding the many levels of neuro-functional organization of the nervous system, specifically peripheral nerves and spinal segments at dermatomes, myotomes and sclerotomes, including which divisions (anterior or posterior), what vertebral levels and what viscera are associated with those spinal seg-ments. Neurofunctional diagnosis is an ambitious clinical approach, but is the best we have in order to help generate the most effective therapeutic interven-tions available for the millions of sufferers with these pain with move-ment disorders.
Chiropractic + Naturopathic Doctor May 2018: Page 16