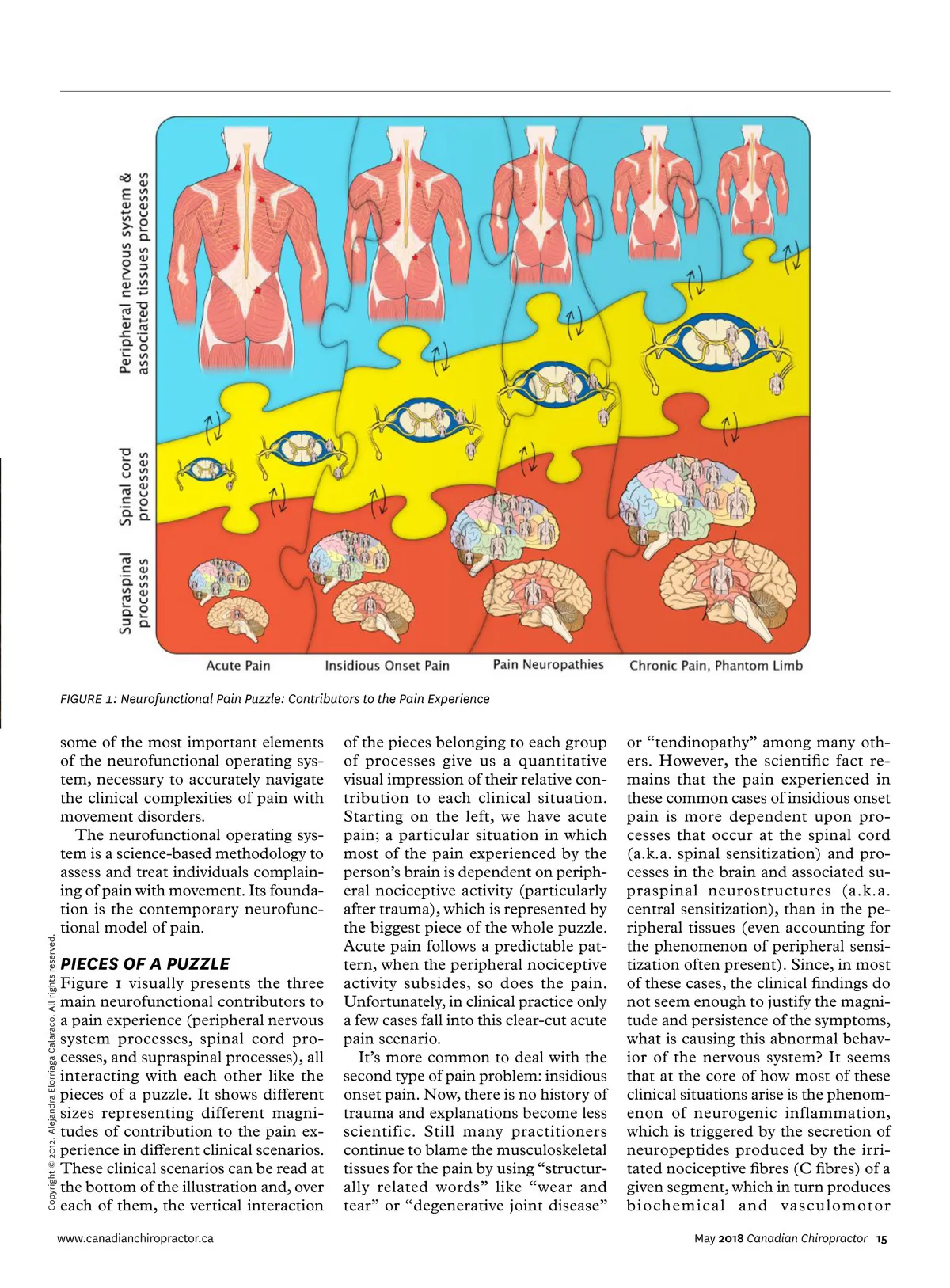
FIGURE 1: Neurofunctional Pain Puzzle: Contributors to the Pain Experience Copyright © 2012. Alejandra Elorriaga Calaraco. All rights reserved. some of the most important elements of the neurofunctional operating sys-tem, necessary to accurately navigate the clinical complexities of pain with movement disorders. The neurofunctional operating sys-tem is a science-based methodology to assess and treat individuals complain-ing of pain with movement. Its founda-tion is the contemporary neurofunc-tional model of pain. PIECES OF A PUZZLE Figure 1 visually presents the three main neurofunctional contributors to a pain experience (peripheral nervous system processes, spinal cord pro-cesses, and supraspinal processes), all interacting with each other like the pieces of a puzzle. It shows different sizes representing different magni-tudes of contribution to the pain ex-perience in different clinical scenarios. These clinical scenarios can be read at the bottom of the illustration and, over each of them, the vertical interaction www.canadianchiropractor.ca of the pieces belonging to each group of processes give us a quantitative visual impression of their relative con-tribution to each clinical situation. Starting on the left, we have acute pain; a particular situation in which most of the pain experienced by the person’s brain is dependent on periph-eral nociceptive activity (particularly after trauma), which is represented by the biggest piece of the whole puzzle. Acute pain follows a predictable pat-tern, when the peripheral nociceptive activity subsides, so does the pain. Unfortunately, in clinical practice only a few cases fall into this clear-cut acute pain scenario. It’s more common to deal with the second type of pain problem: insidious onset pain. Now, there is no history of trauma and explanations become less scientific. Still many practitioners continue to blame the musculoskeletal tissues for the pain by using “structur-ally related words” like “wear and tear” or “degenerative joint disease” or “tendinopathy” among many oth-ers. However, the scientific fact re-mains that the pain experienced in these common cases of insidious onset pain is more dependent upon pro-cesses that occur at the spinal cord (a.k.a. spinal sensitization) and pro-cesses in the brain and associated su-praspinal neurostructures (a.k.a. central sensitization), than in the pe-ripheral tissues (even accounting for the phenomenon of peripheral sensi-tization often present). Since, in most of these cases, the clinical findings do not seem enough to justify the magni-tude and persistence of the symptoms, what is causing this abnormal behav-ior of the nervous system? It seems that at the core of how most of these clinical situations arise is the phenom-enon of neurogenic inflammation, which is triggered by the secretion of neuropeptides produced by the irri-tated nociceptive fibres (C fibres) of a given segment, which in turn produces biochemical and vasculomotor May 2018 Canadian Chiropractor 15
Chiropractic + Naturopathic Doctor May 2018: Page 15