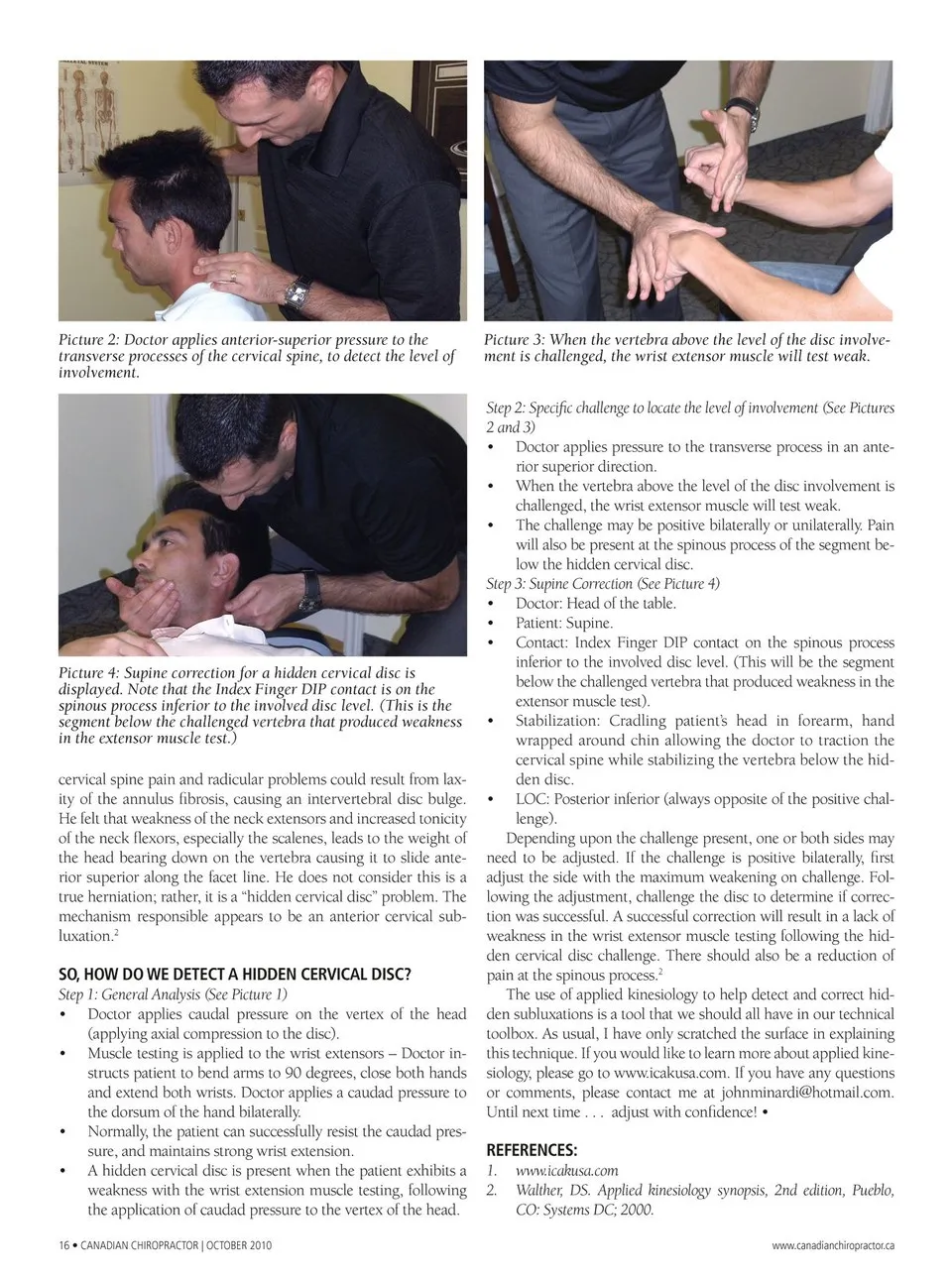
Picture 2: Doctor applies anterior-superior pressure to the transverse processes of the cervical spine, to detect the level of involvement. Picture 3: When the vertebra above the level of the disc involve-ment is challenged, the wrist extensor muscle will test weak. Step 2: Specific challenge to locate the level of involvement (See Pictures 2 and 3) • Doctor applies pressure to the transverse process in an ante-rior superior direction. • When the vertebra above the level of the disc involvement is challenged, the wrist extensor muscle will test weak. Picture 4: Supine correction for a hidden cervical disc is displayed. Note that the Index Finger DIP contact is on the spinous process inferior to the involved disc level. (This is the segment below the challenged vertebra that produced weakness in the extensor muscle test.) cervical spine pain and radicular problems could result from lax-ity of the annulus fibrosis, causing an intervertebral disc bulge. He felt that weakness of the neck extensors and increased tonicity of the neck flexors, especially the scalenes, leads to the weight of the head bearing down on the vertebra causing it to slide ante-rior superior along the facet line. He does not consider this is a true herniation; rather, it is a “hidden cervical disc” problem. The mechanism responsible appears to be an anterior cervical sub-luxation.2 SO,HOW DO WE DETECT A HIDDEN CERVICAL DISC? Step 1: General Analysis (See Picture 1) • Doctor applies caudal pressure on the vertex of the head (applying axial compression to the disc). • Muscle testing is applied to the wrist extensors – Doctor in-structs patient to bend arms to 90 degrees, close both hands and extend both wrists. Doctor applies a caudad pressure to the dorsum of the hand bilaterally. • Normally, the patient can successfully resist the caudad pres-sure, and maintains strong wrist extension. • A hidden cervical disc is present when the patient exhibits a weakness with the wrist extension muscle testing, following the application of caudad pressure to the vertex of the head. 16 • CANADIAN CHIROPRACTOR | OCTOBER 2010 • The challenge may be positive bilaterally or unilaterally. Pain will also be present at the spinous process of the segment be-low the hidden cervical disc. Step 3: Supine Correction (See Picture 4) • Doctor: Head of the table. • Patient: Supine. • Contact: Index Finger DIP contact on the spinous process inferior to the involved disc level. (This will be the segment below the challenged vertebra that produced weakness in the extensor muscle test). • Stabilization: Cradling patient’s head in forearm, hand wrapped around chin allowing the doctor to traction the cervical spine while stabilizing the vertebra below the hid-den disc. • LOC: Posterior inferior (always opposite of the positive chal-lenge). Depending upon the challenge present, one or both sides may need to be adjusted. If the challenge is positive bilaterally, first adjust the side with the maximum weakening on challenge. Fol-lowing the adjustment, challenge the disc to determine if correc-tion was successful. A successful correction will result in a lack of weakness in the wrist extensor muscle testing following the hid-den cervical disc challenge. There should also be a reduction of pain at the spinous process.2 The use of applied kinesiology to help detect and correct hid-den subluxations is a tool that we should all have in our technical toolbox. As usual, I have only scratched the surface in explaining this technique. If you would like to learn more about applied kine-siology, please go to www.icakusa.com. If you have any questions or comments, please contact me at [email protected]. Until next time . . . adjust with confidence! • REFERENCES: 1. www.icakusa.com 2. Walther, DS. Applied kinesiology synopsis, 2nd edition, Pueblo, CO: Systems DC; 2000. www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor October 2010: Page 16