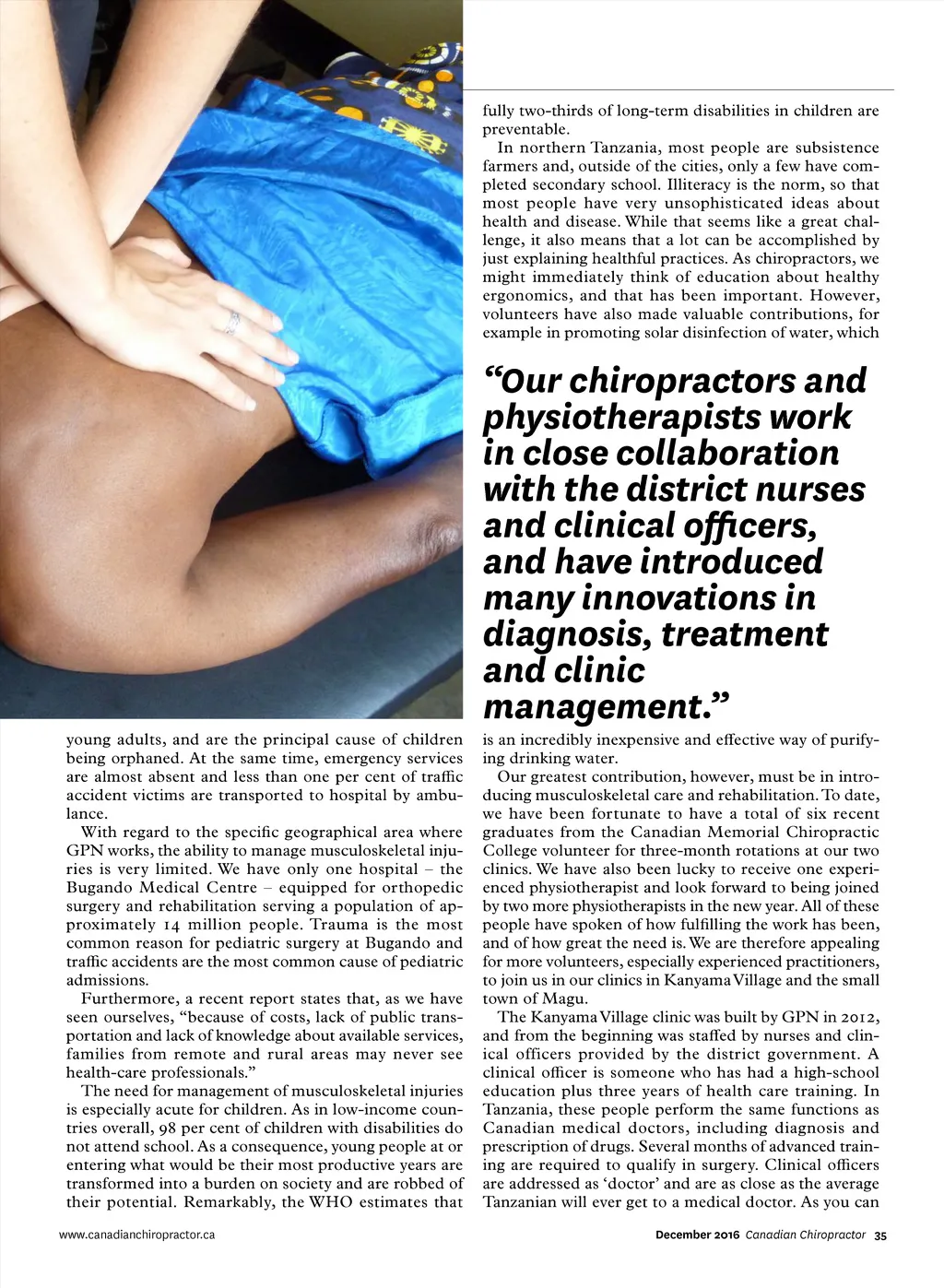
fully two-thirds of long-term disabilities in children are preventable. In northern Tanzania, most people are subsistence farmers and, outside of the cities, only a few have com-pleted secondary school. Illiteracy is the norm, so that most people have very unsophisticated ideas about health and disease. While that seems like a great chal-lenge, it also means that a lot can be accomplished by just explaining healthful practices. As chiropractors, we might immediately think of education about healthy ergonomics, and that has been important. However, volunteers have also made valuable contributions, for example in promoting solar disinfection of water, which “Our chiropractors and physiotherapists work in close collaboration with the district nurses and clinical officers, and have introduced many innovations in diagnosis, treatment and clinic management.” young adults, and are the principal cause of children being orphaned. At the same time, emergency services are almost absent and less than one per cent of traffic accident victims are transported to hospital by ambu-lance. With regard to the specific geographical area where GPN works, the ability to manage musculoskeletal inju-ries is very limited. We have only one hospital – the Bugando Medical Centre – equipped for orthopedic surgery and rehabilitation serving a population of ap-proximately 14 million people. Trauma is the most common reason for pediatric surgery at Bugando and traffic accidents are the most common cause of pediatric admissions. Furthermore, a recent report states that, as we have seen ourselves, “because of costs, lack of public trans-portation and lack of knowledge about available services, families from remote and rural areas may never see health-care professionals.” The need for management of musculoskeletal injuries is especially acute for children. As in low-income coun-tries overall, 98 per cent of children with disabilities do not attend school. As a consequence, young people at or entering what would be their most productive years are transformed into a burden on society and are robbed of their potential. Remarkably, the WHO estimates that www.canadianchiropractor.ca is an incredibly inexpensive and effective way of purify-ing drinking water. Our greatest contribution, however, must be in intro-ducing musculoskeletal care and rehabilitation. To date, we have been fortunate to have a total of six recent graduates from the Canadian Memorial Chiropractic College volunteer for three-month rotations at our two clinics. We have also been lucky to receive one experi-enced physiotherapist and look forward to being joined by two more physiotherapists in the new year. All of these people have spoken of how fulfilling the work has been, and of how great the need is. We are therefore appealing for more volunteers, especially experienced practitioners, to join us in our clinics in Kanyama Village and the small town of Magu. The Kanyama Village clinic was built by GPN in 2012, and from the beginning was staffed by nurses and clin-ical officers provided by the district government. A clinical officer is someone who has had a high-school education plus three years of health care training. In Tanzania, these people perform the same functions as Canadian medical doctors, including diagnosis and prescription of drugs. Several months of advanced train-ing are required to qualify in surgery. Clinical officers are addressed as ‘doctor’ and are as close as the average Tanzanian will ever get to a medical doctor. As you can December 2016 Canadian Chiropractor 35
Chiropractic + Naturopathic Doctor December 2016: Page 35