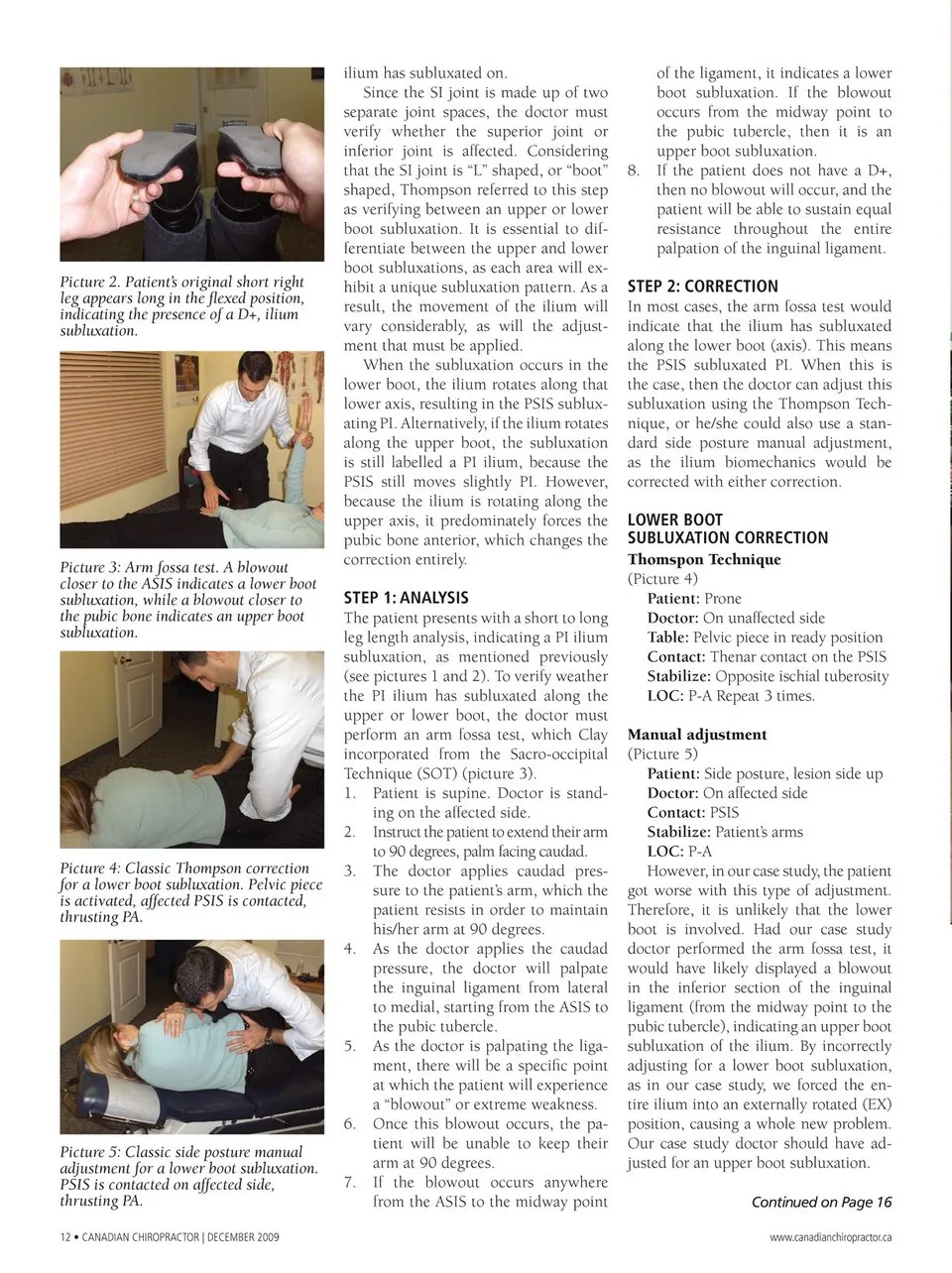
ilium has subluxated on. Since the SI joint is made up of two Picture 2. Patient’s original short right leg appears long in the flexed position, indicating the presence of a D+, ilium subluxation. separate joint spaces, the doctor must verify whether the superior joint or inferior joint is affected. Considering that the SI joint is “L” shaped, or “boot” shaped, Thompson referred to this step as verifying between an upper or lower boot subluxation. It is essential to dif- ferentiate between the upper and lower boot subluxations, as each area will ex- hibit a unique subluxation pattern. As a result, the movement of the ilium will vary considerably, as will the adjust- ment that must be applied. When the subluxation occurs in the Picture 3: Arm fossa test. A blowout closer to the ASIS indicates a lower boot subluxation, while a blowout closer to the pubic bone indicates an upper boot subluxation. lower boot, the ilium rotates along that lower axis, resulting in the PSIS sublux- ating PI. Alternatively, if the ilium rotates along the upper boot, the subluxation is still labelled a PI ilium, because the PSIS still moves slightly PI. However, because the ilium is rotating along the upper axis, it predominately forces the pubic bone anterior, which changes the correction entirely. Picture 4: Classic Thompson correction for a lower boot subluxation. Pelvic piece is activated, affected PSIS is contacted, thrusting PA. Picture 5: Classic side posture manual adjustment for a lower boot subluxation. PSIS is contacted on affected side, thrusting PA. 12 • Canadian ChiropraCtor | dECEMBEr 2009 STEP 1: ANALYSIS The patient presents with a short to long leg length analysis, indicating a PI ilium subluxation, as mentioned previously (see pictures 1 and 2). To verify weather the PI ilium has subluxated along the upper or lower boot, the doctor must perform an arm fossa test, which Clay incorporated from the Sacro-occipital Technique (SOT) (picture 3). 1. Patient is supine. Doctor is stand- ing on the affected side. 2. Instruct the patient to extend their arm to 90 degrees, palm facing caudad. 3. The doctor applies caudad pres- sure to the patient’s arm, which the patient resists in order to maintain his/her arm at 90 degrees. 4. As the doctor applies the caudad pressure, the doctor will palpate the inguinal ligament from lateral to medial, starting from the ASIS to the pubic tubercle. 5. As the doctor is palpating the liga- ment, there will be a specific point at which the patient will experience a “blowout” or extreme weakness. 6. Once this blowout occurs, the pa- tient will be unable to keep their arm at 90 degrees. 7. If the blowout occurs anywhere from the ASIS to the midway point of the ligament, it indicates a lower boot subluxation. If the blowout occurs from the midway point to the pubic tubercle, then it is an upper boot subluxation. 8. If the patient does not have a D+, then no blowout will occur, and the patient will be able to sustain equal resistance throughout the entire palpation of the inguinal ligament. STEP 2: CORRECTION In most cases, the arm fossa test would indicate that the ilium has subluxated along the lower boot (axis). This means the PSIS subluxated PI. When this is the case, then the doctor can adjust this subluxation using the Thompson Tech- nique, or he/she could also use a stan- dard side posture manual adjustment, as the ilium biomechanics would be corrected with either correction. LOWER bOOT SUbLUXATION CORRECTION Thomspon Technique (Picture 4) Patient: Prone Doctor: On unaffected side Table: Pelvic piece in ready position Contact: Thenar contact on the PSIS Stabilize: Opposite ischial tuberosity LOC: P-A Repeat 3 times. Manual adjustment (Picture 5) Patient: Side posture, lesion side up Doctor: On affected side Contact: PSIS Stabilize: Patient’s arms LOC: P-A However, in our case study, the patient got worse with this type of adjustment. Therefore, it is unlikely that the lower boot is involved. Had our case study doctor performed the arm fossa test, it would have likely displayed a blowout in the inferior section of the inguinal ligament (from the midway point to the pubic tubercle), indicating an upper boot subluxation of the ilium. By incorrectly adjusting for a lower boot subluxation, as in our case study, we forced the en- tire ilium into an externally rotated (EX) position, causing a whole new problem. Our case study doctor should have ad- justed for an upper boot subluxation. Continued on Page 16 www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor December 2009: Page 12