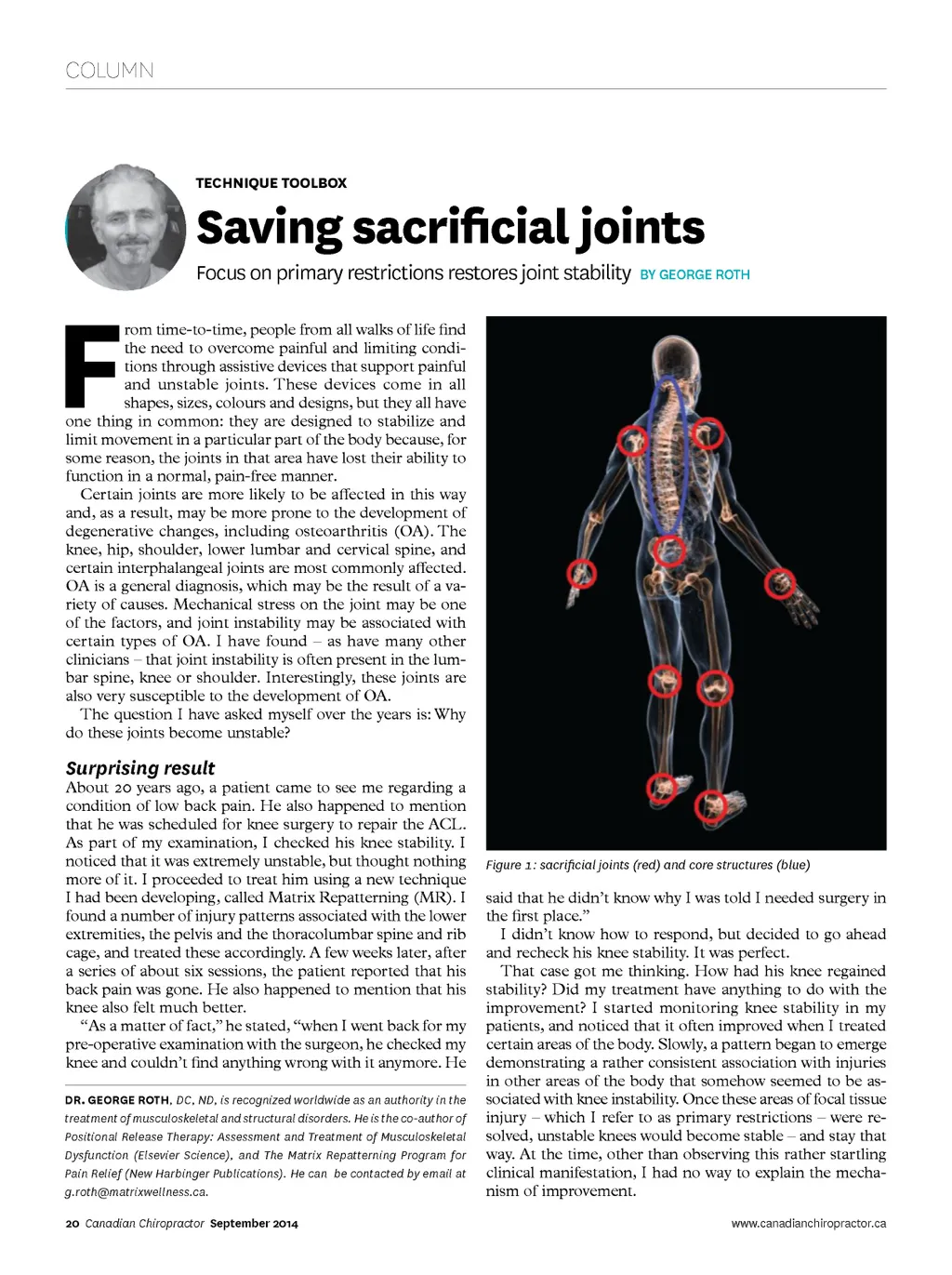
COLUMN TECHNIQUE TOOLBOX Saving sacrificial joints F Focus on primary restrictions restores joint stability BY GEORGE ROTH rom time-to-time, people from all walks of life find the need to overcome painful and limiting condi-tions through assistive devices that support painful and unstable joints. These devices come in all shapes, sizes, colours and designs, but they all have one thing in common: they are designed to stabilize and limit movement in a particular part of the body because, for some reason, the joints in that area have lost their ability to function in a normal, pain-free manner. Certain joints are more likely to be affected in this way and, as a result, may be more prone to the development of degenerative changes, including osteoarthritis (OA). The knee, hip, shoulder, lower lumbar and cervical spine, and certain interphalangeal joints are most commonly affected. OA is a general diagnosis, which may be the result of a va-riety of causes. Mechanical stress on the joint may be one of the factors, and joint instability may be associated with certain types of OA. I have found – as have many other clinicians – that joint instability is often present in the lum-bar spine, knee or shoulder. Interestingly, these joints are also very susceptible to the development of OA. The question I have asked myself over the years is: Why do these joints become unstable? Surprising result About 20 years ago, a patient came to see me regarding a condition of low back pain. He also happened to mention that he was scheduled for knee surgery to repair the ACL. As part of my examination, I checked his knee stability. I noticed that it was extremely unstable, but thought nothing more of it. I proceeded to treat him using a new technique I had been developing, called Matrix Repatterning (MR). I found a number of injury patterns associated with the lower extremities, the pelvis and the thoracolumbar spine and rib cage, and treated these accordingly. A few weeks later, after a series of about six sessions, the patient reported that his back pain was gone. He also happened to mention that his knee also felt much better. “As a matter of fact,” he stated, “when I went back for my pre-operative examination with the surgeon, he checked my knee and couldn’t find anything wrong with it anymore. He DR. GEORGE ROTH , DC, ND, is recognized worldwide as an authority in the treatment of musculoskeletal and structural disorders. He is the co-author of Positional Release Therapy: Assessment and Treatment of Musculoskeletal Dysfunction (Elsevier Science), and The Matrix Repatterning Program for Pain Relief (New Harbinger Publications). He can be contacted by email at [email protected]. 20 Canadian Chiropractor September 2014 Figure 1: sacrificial joints (red) and core structures (blue) said that he didn’t know why I was told I needed surgery in the first place.” I didn’t know how to respond, but decided to go ahead and recheck his knee stability. It was perfect. That case got me thinking. How had his knee regained stability? Did my treatment have anything to do with the improvement? I started monitoring knee stability in my patients, and noticed that it often improved when I treated certain areas of the body. Slowly, a pattern began to emerge demonstrating a rather consistent association with injuries in other areas of the body that somehow seemed to be as-sociated with knee instability. Once these areas of focal tissue injury – which I refer to as primary restrictions – were re-solved, unstable knees would become stable – and stay that way. At the time, other than observing this rather startling clinical manifestation, I had no way to explain the mecha-nism of improvement. www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor September 2014: Page 20