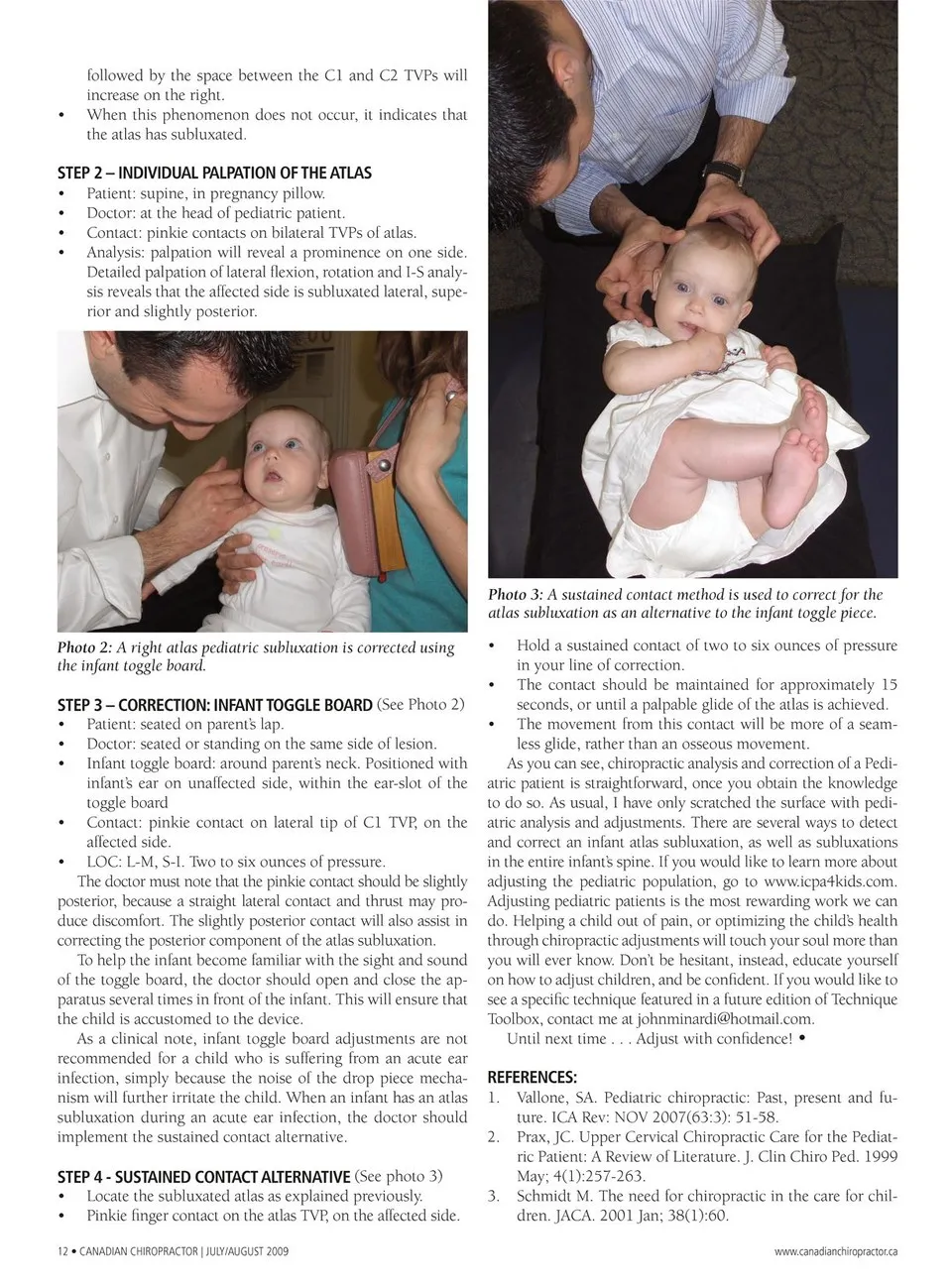
followed by the space between the C1 and C2 TVPs will increase on the right. • • • • • When this phenomenon does not occur, it indicates that the atlas has subluxated. STEP 2 – INDIVIDUAL PALPATION OF THE ATLAS Patient: supine, in pregnancy pillow. Doctor: at the head of pediatric patient. Contact: pinkie contacts on bilateral TVPs of atlas. Analysis: palpation will reveal a prominence on one side. Detailed palpation of lateral fl exion, rotation and I-S analy- sis reveals that the affected side is subluxated lateral, supe- rior and slightly posterior. Photo 3: A sustained contact method is used to correct for the atlas subluxation as an alternative to the infant toggle piece. Photo 2: A right atlas pediatric subluxation is corrected using the infant toggle board. • • • • • STEP 3 – CORRECTION: INFANT TOGGLE BOARD (See Photo 2) Patient: seated on parent’s lap. Doctor: seated or standing on the same side of lesion. Infant toggle board: around parent’s neck. Positioned with infant’s ear on unaffected side, within the ear-slot of the toggle board Contact: pinkie contact on lateral tip of C1 TVP, on the affected side. LOC: L-M, S-I. Two to six ounces of pressure. The doctor must note that the pinkie contact should be slightly posterior, because a straight lateral contact and thrust may pro- duce discomfort. The slightly posterior contact will also assist in correcting the posterior component of the atlas subluxation. To help the infant become familiar with the sight and sound of the toggle board, the doctor should open and close the ap- paratus several times in front of the infant. This will ensure that the child is accustomed to the device. As a clinical note, infant toggle board adjustments are not recommended for a child who is suffering from an acute ear infection, simply because the noise of the drop piece mecha- nism will further irritate the child. When an infant has an atlas subluxation during an acute ear infection, the doctor should implement the sustained contact alternative. • • STEP 4 - SUSTAINED CONTACT ALTERNATIVE (See photo 3) Locate the subluxated atlas as explained previously. Pinkie fi nger contact on the atlas TVP, on the affected side. 12 • CANADIAN CHIROPRACTOR | JULY/AUGUST 2009 • • • Hold a sustained contact of two to six ounces of pressure in your line of correction. The contact should be maintained for approximately 15 seconds, or until a palpable glide of the atlas is achieved. The movement from this contact will be more of a seam- less glide, rather than an osseous movement. As you can see, chiropractic analysis and correction of a Pedi- atric patient is straightforward, once you obtain the knowledge to do so. As usual, I have only scratched the surface with pedi- atric analysis and adjustments. There are several ways to detect and correct an infant atlas subluxation, as well as subluxations in the entire infant’s spine. If you would like to learn more about adjusting the pediatric population, go to www.icpa4kids.com. Adjusting pediatric patients is the most rewarding work we can do. Helping a child out of pain, or optimizing the child’s health through chiropractic adjustments will touch your soul more than you will ever know. Don’t be hesitant, instead, educate yourself on how to adjust children, and be confi dent. If you would like to see a specifi c technique featured in a future edition of Technique Toolbox, contact me at [email protected]. Until next time . . . Adjust with confidence! • REFERENCES: Vallone, SA. Pediatric chiropractic: Past, present and fu- ture. ICA Rev: NOV 2007(63:3): 51-58. Prax, JC. Upper Cervical Chiropractic Care for the Pediat- ric Patient: A Review of Literature. J. Clin Chiro Ped. 1999 May; 4(1):257-263. 1. 2. 3. Schmidt M. The need for chiropractic in the care for chil- dren. JACA. 2001 Jan; 38(1):60. www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor July/August 2009: Page 12