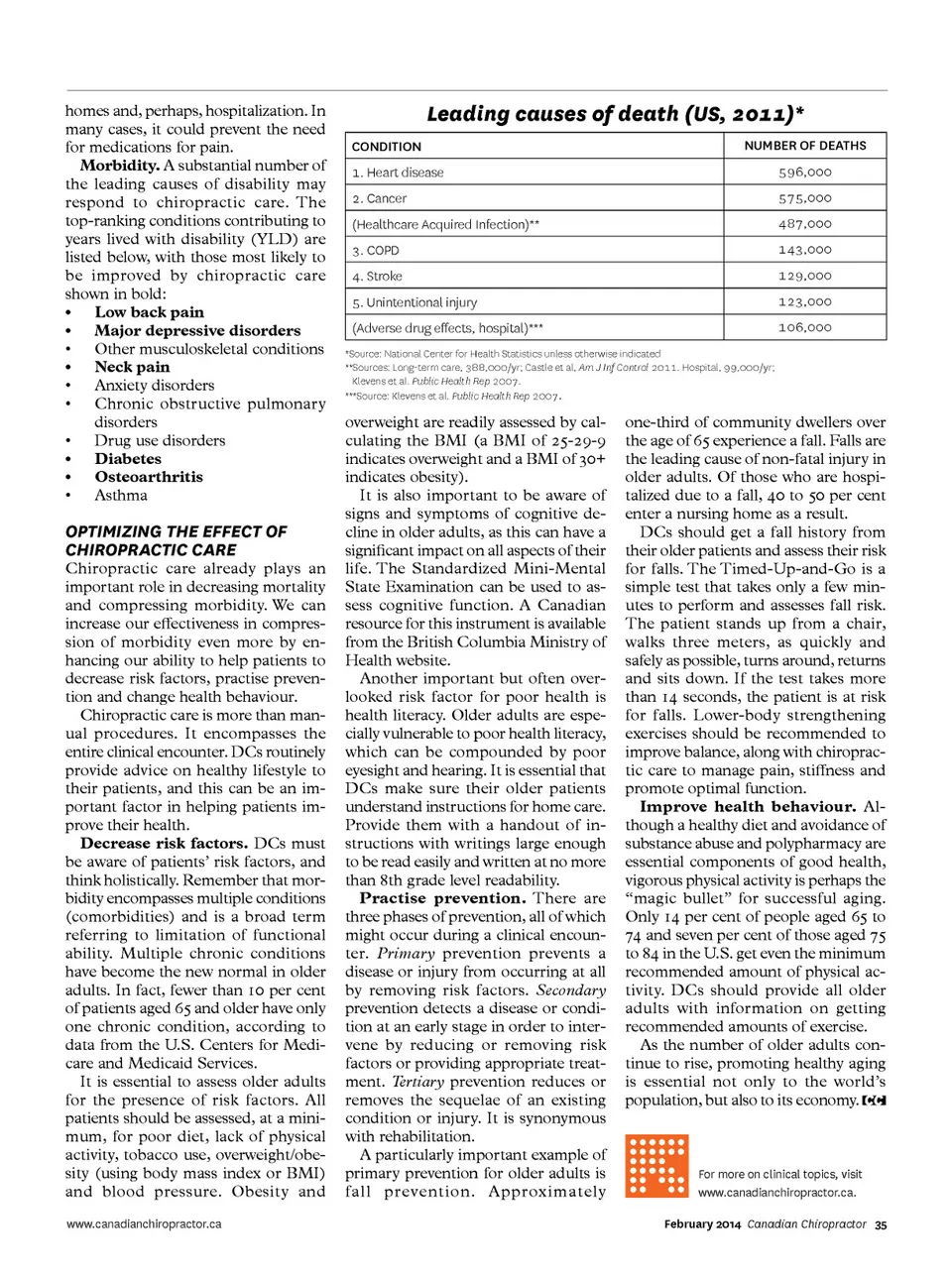
homes and, perhaps, hospitalization. In many cases, it could prevent the need for medications for pain. Morbidity. A substantial number of the leading causes of disability may respond to chiropractic care. The top-ranking conditions contributing to years lived with disability (YLD) are listed below, with those most likely to be improved by chiropractic care shown in bold: • Low back pain • Major depressive disorders • Other musculoskeletal conditions • Neck pain • Anxiety disorders • Chronic obstructive pulmonary disorders • Drug use disorders • Diabetes • Osteoarthritis • Asthma Leading causes of death (Us, 2011)* Condition 1. Heart disease 2. Cancer (Healthcare Acquired Infection)** 3. COPD 4. Stroke 5. Unintentional injury (Adverse drug effects, hospital)*** *Source: National Center for Health Statistics unless otherwise indicated **Sources: Long-term care, 388,000/yr; Castle et al, Am J Inf Control 2011. Hospital, 99,000/yr; Klevens et al. Public Health Rep 2007. ***Source: Klevens et al. Public Health Rep 2007 . nuMber of deaths 596,000 575,000 487,000 143,000 129,000 123,000 106,000 oPTIMIzINg The eFFecT oF chIroPracTIc care Chiropractic care already plays an important role in decreasing mortality and compressing morbidity. We can increase our effectiveness in compres-sion of morbidity even more by en-hancing our ability to help patients to decrease risk factors, practise preven-tion and change health behaviour. Chiropractic care is more than man-ual procedures. It encompasses the entire clinical encounter. DCs routinely provide advice on healthy lifestyle to their patients, and this can be an im-portant factor in helping patients im-prove their health. Decrease risk factors. DCs must be aware of patients’ risk factors, and think holistically. Remember that mor-bidity encompasses multiple conditions (comorbidities) and is a broad term referring to limitation of functional ability. Multiple chronic conditions have become the new normal in older adults. In fact, fewer than 10 per cent of patients aged 65 and older have only one chronic condition, according to data from the U.S. Centers for Medi-care and Medicaid Services. It is essential to assess older adults for the presence of risk factors. All patients should be assessed, at a mini-mum, for poor diet, lack of physical activity, tobacco use, overweight/obe-sity (using body mass index or BMI) and blood pressure. Obesity and www.canadianchiropractor.ca overweight are readily assessed by cal-culating the BMI (a BMI of 25-29-9 indicates overweight and a BMI of 30+ indicates obesity). It is also important to be aware of signs and symptoms of cognitive de-cline in older adults, as this can have a significant impact on all aspects of their life. The Standardized Mini-Mental State Examination can be used to as-sess cognitive function. A Canadian resource for this instrument is available from the British Columbia Ministry of Health website. Another important but often over-looked risk factor for poor health is health literacy. Older adults are espe-cially vulnerable to poor health literacy, which can be compounded by poor eyesight and hearing. It is essential that DCs make sure their older patients understand instructions for home care. Provide them with a handout of in-structions with writings large enough to be read easily and written at no more than 8th grade level readability. Practise prevention. There are three phases of prevention, all of which might occur during a clinical encoun-ter. Primary prevention prevents a disease or injury from occurring at all by removing risk factors. Secondary prevention detects a disease or condi-tion at an early stage in order to inter-vene by reducing or removing risk factors or providing appropriate treat-ment. Tertiary prevention reduces or removes the sequelae of an existing condition or injury. It is synonymous with rehabilitation. A particularly important example of primary prevention for older adults is f all prevention. Approximately one-third of community dwellers over the age of 65 experience a fall. Falls are the leading cause of non-fatal injury in older adults. Of those who are hospi-talized due to a fall, 40 to 50 per cent enter a nursing home as a result. DCs should get a fall history from their older patients and assess their risk for falls. The Timed-Up-and-Go is a simple test that takes only a few min-utes to perform and assesses fall risk. The patient stands up from a chair, walks three meters, as quickly and safely as possible, turns around, returns and sits down. If the test takes more than 14 seconds, the patient is at risk for falls. Lower-body strengthening exercises should be recommended to improve balance, along with chiroprac-tic care to manage pain, stiffness and promote optimal function. Improve health behaviour. Al-though a healthy diet and avoidance of substance abuse and polypharmacy are essential components of good health, vigorous physical activity is perhaps the “magic bullet” for successful aging. Only 14 per cent of people aged 65 to 74 and seven per cent of those aged 75 to 84 in the U.S. get even the minimum recommended amount of physical ac-tivity. DCs should provide all older adults with information on getting recommended amounts of exercise. As the number of older adults con-tinue to rise, promoting healthy aging is essential not only to the world’s population, but also to its economy. For more on clinical topics, visit www.canadianchiropractor.ca. February 2014 Canadian Chiropractor 35
Chiropractic + Naturopathic Doctor February 2014: Page 35