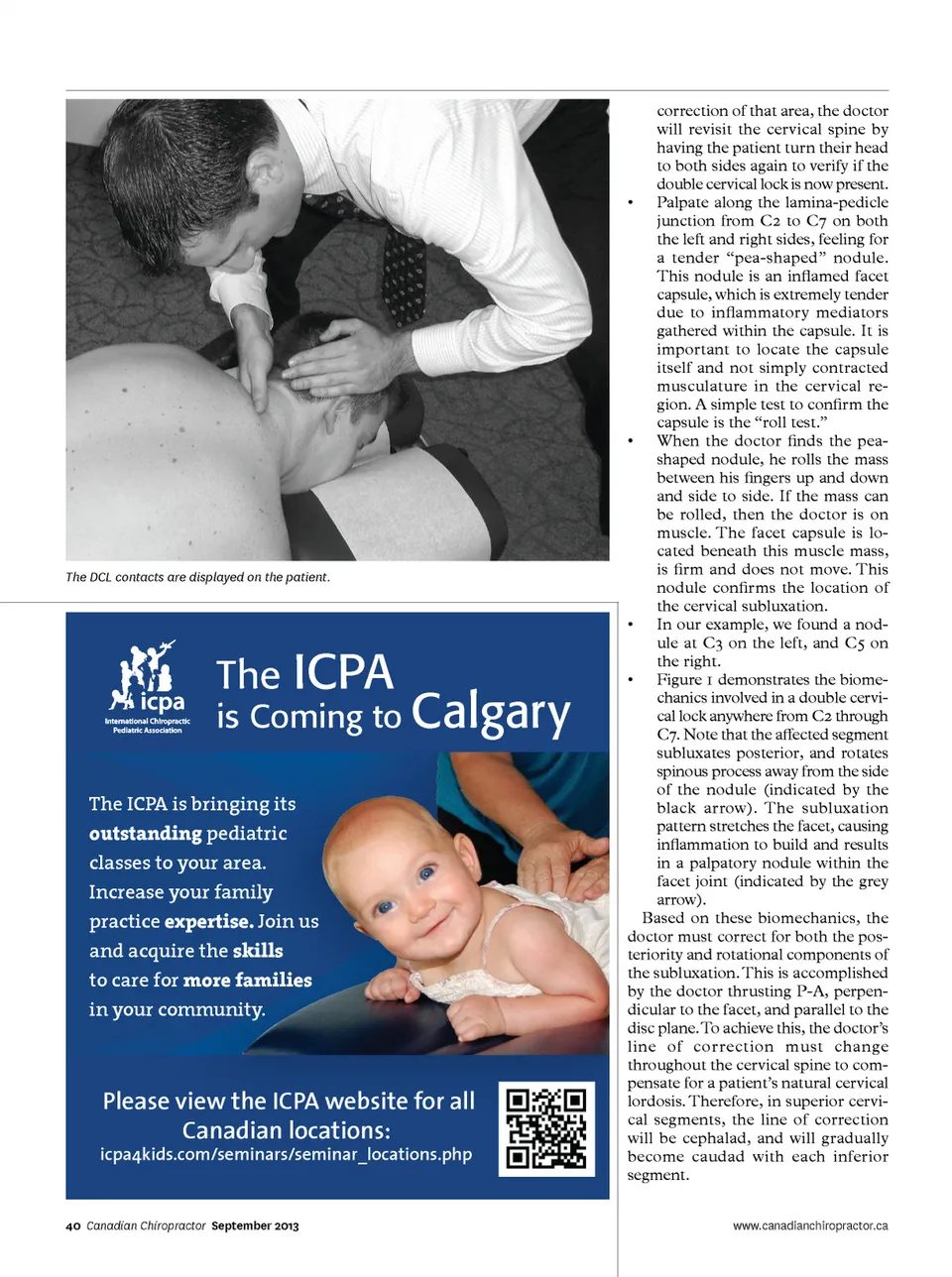
The DCL contacts are displayed on the patient. The is Coming to Calgary The ICPA is bringing its outstanding pediatric classes to your area. Increase your family ICPA practice expertise. Join us and acquire the skills to care for more families in your community. icpa4kids.com/seminars/seminar_locations.php Please view the ICPA website for all Canadian locations: correction of that area, the doctor will revisit the cervical spine by having the patient turn their head to both sides again to verify if the double cervical lock is now present. • Palpate along the lamina-pedicle junction from C2 to C7 on both the left and right sides, feeling for a tender “pea-shaped” nodule. This nodule is an inflamed facet capsule, which is extremely tender due to inflammatory mediators gathered within the capsule. It is important to locate the capsule itself and not simply contracted musculature in the cervical re-gion. A simple test to confirm the capsule is the “roll test.” • When the doctor finds the pea-shaped nodule, he rolls the mass between his fingers up and down and side to side. If the mass can be rolled, then the doctor is on muscle. The facet capsule is lo-cated beneath this muscle mass, is firm and does not move. This nodule confirms the location of the cervical subluxation. • In our example, we found a nod-ule at C3 on the left, and C5 on the right. • Figure 1 demonstrates the biome-chanics involved in a double cervi-cal lock anywhere from C2 through C7. Note that the affected segment subluxates posterior, and rotates spinous process away from the side of the nodule (indicated by the black arrow). The subluxation pattern stretches the facet, causing inflammation to build and results in a palpatory nodule within the facet joint (indicated by the grey arrow). Based on these biomechanics, the doctor must correct for both the pos-teriority and rotational components of the subluxation. This is accomplished by the doctor thrusting P-A, perpen-dicular to the facet, and parallel to the disc plane. To achieve this, the doctor’s line of correction must change throughout the cervical spine to com-pensate for a patient’s natural cervical lordosis. Therefore, in superior cervi-cal segments, the line of correction will be cephalad, and will gradually become caudad with each inferior segment. www.canadianchiropractor.ca 40 Canadian Chiropractor September 2013
Chiropractic + Naturopathic Doctor September 2013: Page 40