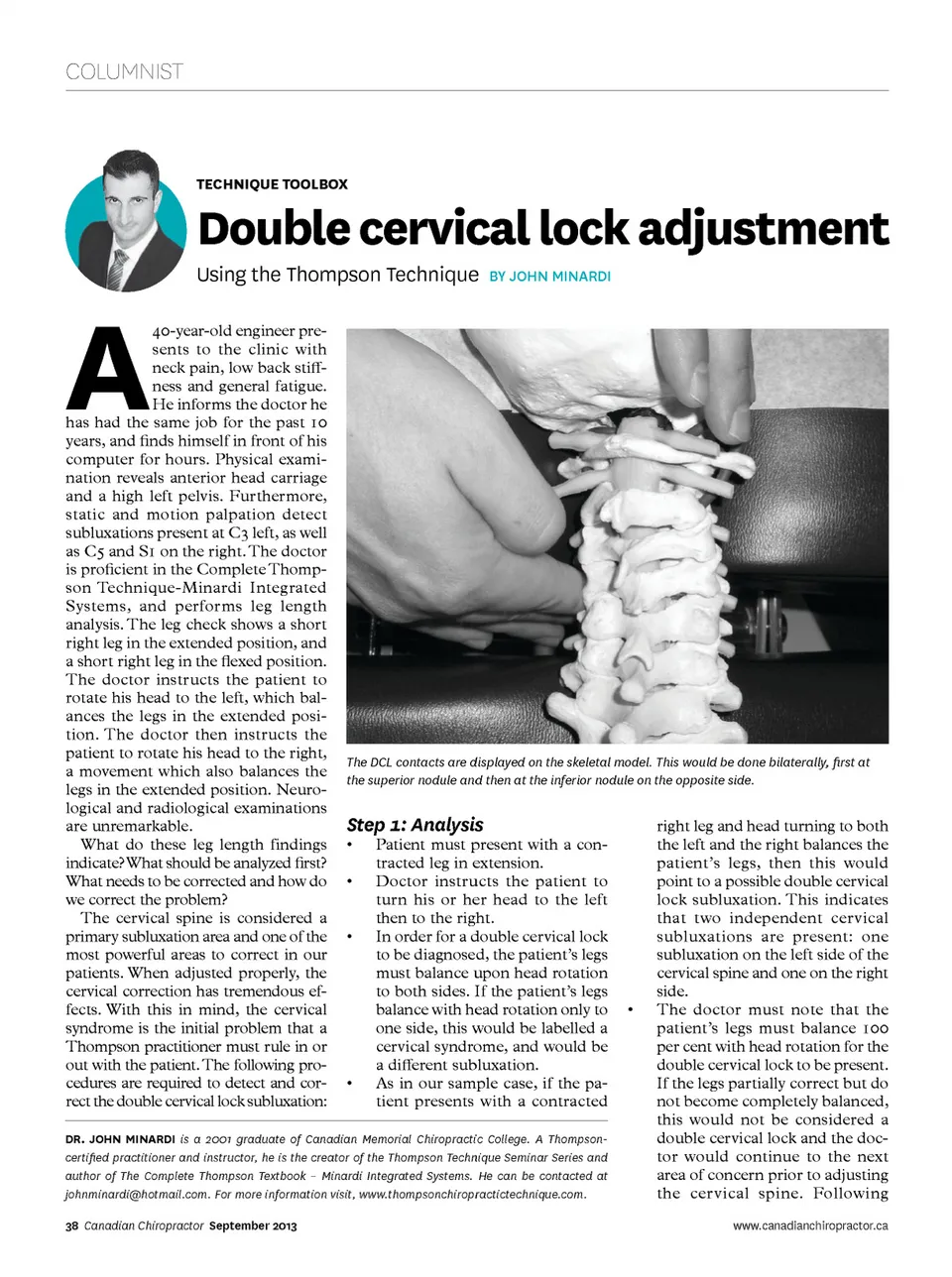
COLUMNIST TECHNIQUE TOOlBOx Double cervical lock adjustment A Using the Thompson Technique by john Minardi 40-year-old engineer pre-sents to the clinic with neck pain, low back stiff-ness and general fatigue. He informs the doctor he has had the same job for the past 10 years, and finds himself in front of his computer for hours. Physical exami-nation reveals anterior head carriage and a high left pelvis. Furthermore, static and motion palpation detect subluxations present at C3 left, as well as C5 and S1 on the right. The doctor is proficient in the Complete Thomp-son Technique-Minardi Integrated Systems, and performs leg length analysis. The leg check shows a short right leg in the extended position, and a short right leg in the flexed position. The doctor instructs the patient to rotate his head to the left, which bal-ances the legs in the extended posi-tion. The doctor then instructs the patient to rotate his head to the right, a movement which also balances the legs in the extended position. Neuro-logical and radiological examinations are unremarkable. What do these leg length findings indicate? What should be analyzed first? What needs to be corrected and how do we correct the problem? The cervical spine is considered a primary subluxation area and one of the most powerful areas to correct in our patients. When adjusted properly, the cervical correction has tremendous ef-fects. With this in mind, the cervical syndrome is the initial problem that a Thompson practitioner must rule in or out with the patient. The following pro-cedures are required to detect and cor-rect the double cervical lock subluxation: The DCL contacts are displayed on the skeletal model. This would be done bilaterally, first at the superior nodule and then at the inferior nodule on the opposite side. Step 1: Analysis • • • • Patient must present with a con-tracted leg in extension. Doctor instructs the patient to turn his or her head to the left then to the right. In order for a double cervical lock to be diagnosed, the patient’s legs must balance upon head rotation to both sides. If the patient’s legs balance with head rotation only to one side, this would be labelled a cervical syndrome, and would be a different subluxation. As in our sample case, if the pa-tient presents with a contracted • dr. John minArdi is a 2001 graduate of Canadian Memorial Chiropractic College. A Thompson-certified practitioner and instructor, he is the creator of the Thompson Technique Seminar Series and author of The Complete Thompson Textbook – Minardi Integrated Systems. He can be contacted at [email protected]. For more information visit, www.thompsonchiropractictechnique.com. 38 Canadian Chiropractor September 2013 right leg and head turning to both the left and the right balances the patient’s legs, then this would point to a possible double cervical lock subluxation. This indicates that two independent cervical subluxations are present: one subluxation on the left side of the cervical spine and one on the right side. The doctor must note that the patient’s legs must balance 100 per cent with head rotation for the double cervical lock to be present. If the legs partially correct but do not become completely balanced, this would not be considered a double cervical lock and the doc-tor would continue to the next area of concern prior to adjusting the cervical spine. Following www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor September 2013: Page 38