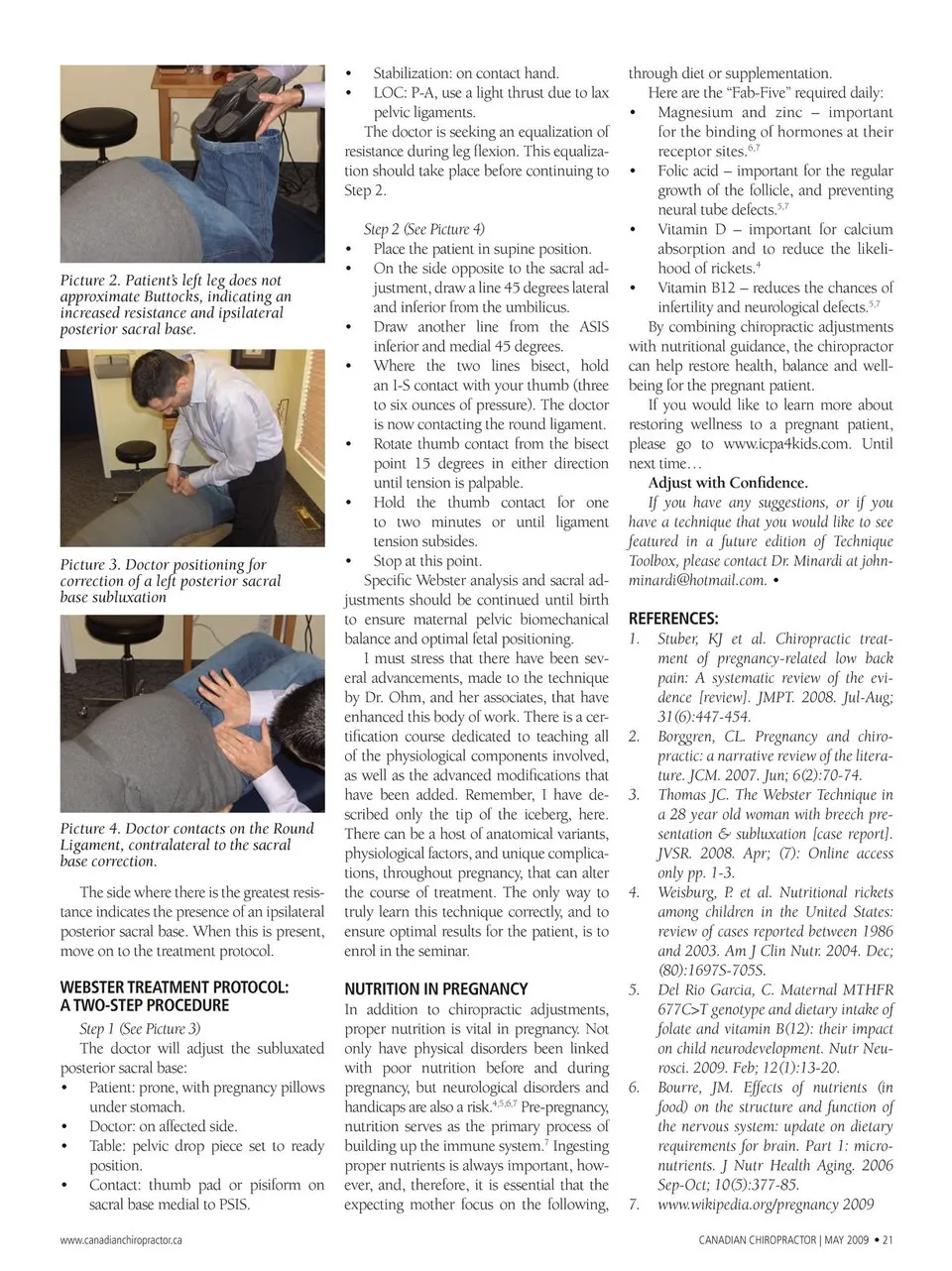
• • Stabilization: on contact hand. LOC: P-A, use a light thrust due to lax pelvic ligaments. The doctor is seeking an equalization of resistance during leg fl exion. This equaliza- tion should take place before continuing to Step 2. Step 2 (See Picture 4) Picture 2. Patient’s left leg does not approximate Buttocks, indicating an increased resistance and ipsilateral posterior sacral base. • • • • Picture 3. Doctor positioning for correction of a left posterior sacral base subluxation • • • Place the patient in supine position. On the side opposite to the sacral ad- justment, draw a line 45 degrees lateral and inferior from the umbilicus. Draw another line from the ASIS inferior and medial 45 degrees. Where the two lines bisect, hold an I-S contact with your thumb (three to six ounces of pressure). The doctor is now contacting the round ligament. Rotate thumb contact from the bisect point 15 degrees in either direction until tension is palpable. Picture 4. Doctor contacts on the Round Ligament, contralateral to the sacral base correction. The side where there is the greatest resis- tance indicates the presence of an ipsilateral posterior sacral base. When this is present, move on to the treatment protocol. WEBSTER TREATMENT PROTOCOL: A TWO-STEP PROCEDURE Step 1 (See Picture 3) The doctor will adjust the subluxated posterior sacral base: Patient: prone, with pregnancy pillows under stomach. Doctor: on affected side. Table: pelvic drop piece set to ready position. • • • • Contact: thumb pad or pisiform on sacral base medial to PSIS. www.canadianchiropractor.ca Hold the thumb contact for one to two minutes or until ligament tension subsides. Stop at this point. Specifi c Webster analysis and sacral ad- justments should be continued until birth to ensure maternal pelvic biomechanical balance and optimal fetal positioning. I must stress that there have been sev- eral advancements, made to the technique by Dr. Ohm, and her associates, that have enhanced this body of work. There is a cer- tifi cation course dedicated to teaching all of the physiological components involved, as well as the advanced modifications that have been added. Remember, I have de- scribed only the tip of the iceberg, here. There can be a host of anatomical variants, physiological factors, and unique complica- tions, throughout pregnancy, that can alter the course of treatment. The only way to truly learn this technique correctly, and to ensure optimal results for the patient, is to enrol in the seminar. NUTRITION IN PREGNANCY In addition to chiropractic adjustments, proper nutrition is vital in pregnancy. Not only have physical disorders been linked with poor nutrition before and during pregnancy, but neurological disorders and handicaps are also a risk.4,5,6,7 nutrition serves as the primary process of building up the immune system.7 Pre-pregnancy, Ingesting proper nutrients is always important, how- ever, and, therefore, it is essential that the expecting mother focus on the following, through diet or supplementation. Here are the “Fab-Five” required daily: Magnesium and zinc – important for the binding of hormones at their receptor sites.6,7 • • • • Folic acid – important for the regular growth of the follicle, and preventing neural tube defects.5,7 Vitamin D – important for calcium absorption and to reduce the likeli- hood of rickets.4 Vitamin B12 – reduces the chances of infertility and neurological defects.5,7 By combining chiropractic adjustments with nutritional guidance, the chiropractor can help restore health, balance and well- being for the pregnant patient. If you would like to learn more about restoring wellness to a pregnant patient, please go to www.icpa4kids.com. Until next time… Adjust with Confidence. If you have any suggestions, or if you have a technique that you would like to see featured in a future edition of Technique Toolbox, please contact Dr. Minardi at john- [email protected]. • REFERENCES: Stuber, KJ et al. Chiropractic treat- ment of pregnancy-related low back pain: A systematic review of the evi- dence [review]. JMPT. 2008. Jul-Aug; 31(6):447-454. Borggren, CL. Pregnancy and chiro- practic: a narrative review of the litera- ture. JCM. 2007. Jun; 6(2):70-74. Thomas JC. The Webster Technique in a 28 year old woman with breech pre- sentation & subluxation [case report]. JVSR. 2008. Apr; (7): Online access only pp. 1-3. Weisburg, P. et al. Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003. Am J Clin Nutr. 2004. Dec; (80):1697S-705S. Del Rio Garcia, C. Maternal MTHFR 677C>T genotype and dietary intake of folate and vitamin B(12): their impact on child neurodevelopment. Nutr Neu- rosci. 2009. Feb; 12(1):13-20. Bourre, JM. Effects of nutrients (in food) on the structure and function of the nervous system: update on dietary requirements for brain. Part 1: micro- nutrients. J Nutr Health Aging. 2006 Sep-Oct; 10(5):377-85. www.wikipedia.org/pregnancy 2009 1. 2. 3. 4. 5. 6. 7. CANADIAN CHIROPRACTOR | MAY 2009 • 21
Chiropractic + Naturopathic Doctor May 2009: Page 21