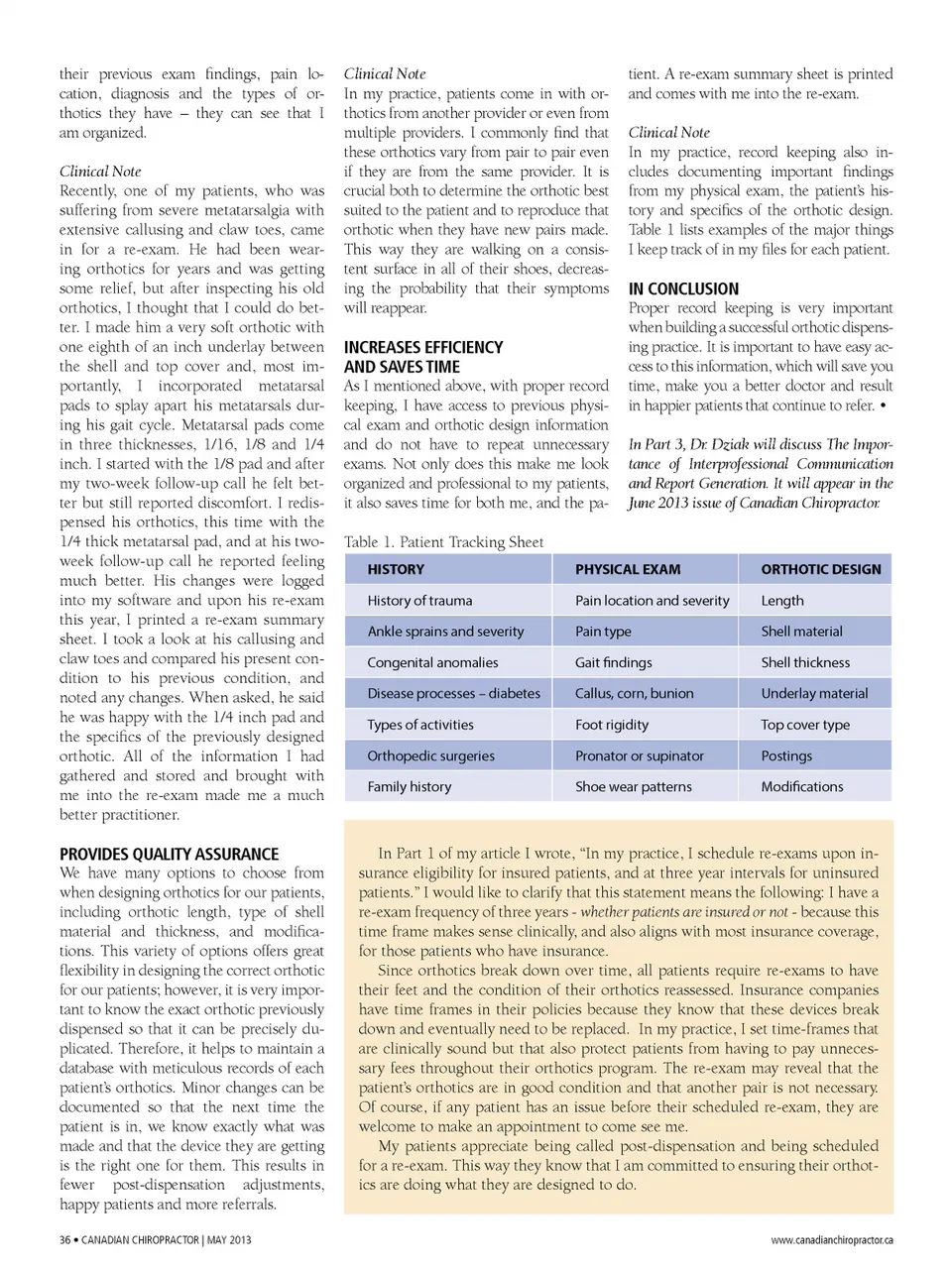
their previous exam findings, pain lo -cation, diagnosis and the types of or -thotics they have – they can see that I am organized. Clinical Note Recently, one of my patients, who was suffering from severe metatarsalgia with extensive callusing and claw toes, came in for a re-exam. He had been wear -ing orthotics for years and was getting some relief, but after inspecting his old orthotics, I thought that I could do bet -ter. I made him a very soft orthotic with one eighth of an inch underlay between the shell and top cover and, most im -portantly, I incorporated metatarsal pads to splay apart his metatarsals dur -ing his gait cycle. Metatarsal pads come in three thicknesses, 1/16, 1/8 and 1/4 inch. I started with the 1/8 pad and after my two-week follow-up call he felt bet -ter but still reported discomfort. I redis -pensed his orthotics, this time with the 1/4 thick metatarsal pad, and at his two-week follow-up call he reported feeling much better. His changes were logged into my software and upon his re-exam this year, I printed a re-exam summary sheet. I took a look at his callusing and claw toes and compared his present con -dition to his previous condition, and noted any changes. When asked, he said he was happy with the 1/4 inch pad and the specifics of the previously designed orthotic. All of the information I had gathered and stored and brought with me into the re-exam made me a much better practitioner. Clinical Note In my practice, patients come in with or -thotics from another provider or even from multiple providers. I commonly find that these orthotics vary from pair to pair even if they are from the same provider. It is crucial both to determine the orthotic best suited to the patient and to reproduce that orthotic when they have new pairs made. This way they are walking on a consis -tent surface in all of their shoes, decreas -ing the probability that their symptoms will reappear. tient. A re-exam summary sheet is printed and comes with me into the re-exam. Clinical Note In my practice, record keeping also in -cludes documenting important findings from my physical exam, the patient’s his -tory and specifics of the orthotic design. Table 1 lists examples of the major things I keep track of in my files for each patient. INCREASES EFFICIENCY AND SAvES TIME As I mentioned above, with proper record keeping, I have access to previous physi -cal exam and orthotic design information and do not have to repeat unnecessary exams. Not only does this make me look organized and professional to my patients, it also saves time for both me, and the pa -Table 1. Patient Tracking Sheet HISTORY History of trauma Ankle sprains and severity Congenital anomalies Disease processes – diabetes Types of activities Orthopedic surgeries Family history IN CONCLuSION Proper record keeping is very important when building a successful orthotic dispens -ing practice. It is important to have easy ac -cess to this information, which will save you time, make you a better doctor and result in happier patients that continue to refer. • In Part 3, Dr. Dziak will discuss The Impor-tance of Interprofessional Communication and Report Generation. It will appear in the June 2013 issue of Canadian Chiropractor. PHYSICAL EXAM Pain location and severity Pain type Gait findings Callus, corn, bunion Foot rigidity Pronator or supinator Shoe wear patterns ORTHOTIC DESIGN Length Shell material Shell thickness Underlay material Top cover type Postings Modifications PROvIDES QuALITY ASSuRANCE We have many options to choose from when designing orthotics for our patients, including orthotic length, type of shell material and thickness, and modifica -tions. This variety of options offers great flexibility in designing the correct orthotic for our patients; however, it is very impor -tant to know the exact orthotic previously dispensed so that it can be precisely du -plicated. Therefore, it helps to maintain a database with meticulous records of each patient’s orthotics. Minor changes can be documented so that the next time the patient is in, we know exactly what was made and that the device they are getting is the right one for them. This results in fewer post-dispensation adjustments, happy patients and more referrals. 36 • CANADIAN CHIROPRACTOR | MAY 2013 In Part 1 of my article I wrote, “In my practice, I schedule re-exams upon in -surance eligibility for insured patients, and at three year intervals for uninsured patients.” I would like to clarify that this statement means the following: I have a re-exam frequency of three years -whether patients are insured or not -because this time frame makes sense clinically, and also aligns with most insurance coverage, for those patients who have insurance. Since orthotics break down over time, all patients require re-exams to have their feet and the condition of their orthotics reassessed. Insurance companies have time frames in their policies because they know that these devices break down and eventually need to be replaced. In my practice, I set time-frames that are clinically sound but that also protect patients from having to pay unneces -sary fees throughout their orthotics program. The re-exam may reveal that the patient’s orthotics are in good condition and that another pair is not necessary. Of course, if any patient has an issue before their scheduled re-exam, they are welcome to make an appointment to come see me. My patients appreciate being called post-dispensation and being scheduled for a re-exam. This way they know that I am committed to ensuring their orthot -ics are doing what they are designed to do. www.canadianchiropractor.ca
Chiropractic + Naturopathic Doctor May 2013: Page 36