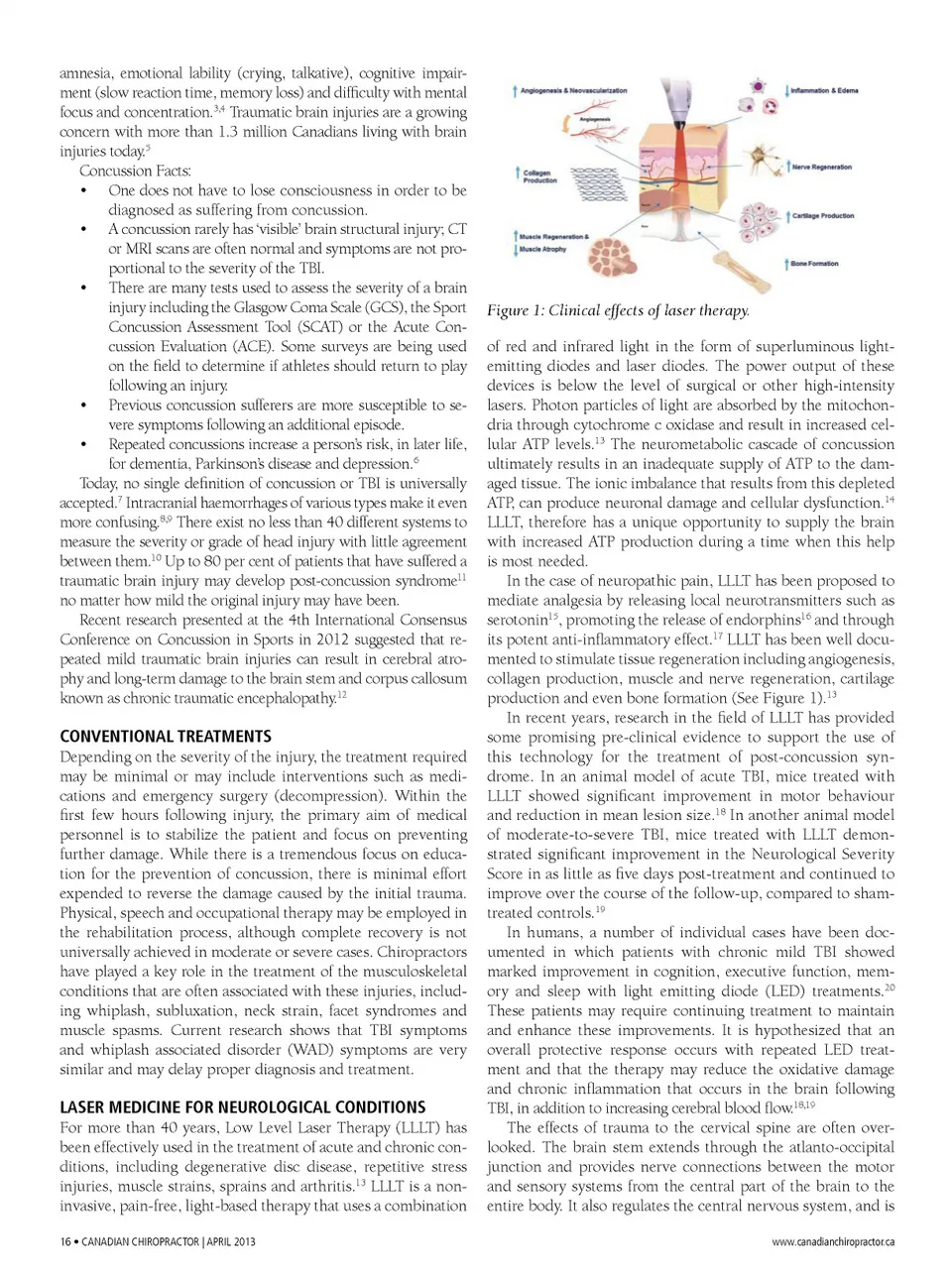
amnesia, emotional lability (crying, talkative), cognitive impair-ment (slow reaction time, memory loss) and difficulty with mental focus and concentration. 3,4 Traumatic brain injuries are a growing concern with more than 1.3 million Canadians living with brain injuries today. 5 Concussion Facts: • One does not have to lose consciousness in order to be diagnosed as suffering from concussion. • A concussion rarely has ‘visible’ brain structural injury; CT or MRI scans are often normal and symptoms are not pro-portional to the severity of the TBI. • There are many tests used to assess the severity of a brain injury including the Glasgow Coma Scale (GCS), the Sport Concussion Assessment Tool (SCAT) or the Acute Con-cussion Evaluation (ACE). Some surveys are being used on the field to determine if athletes should return to play following an injury. • Previous concussion sufferers are more susceptible to se-vere symptoms following an additional episode. • Repeated concussions increase a person’s risk, in later life, for dementia, Parkinson’s disease and depression. 6 Today, no single definition of concussion or TBI is universally accepted. 7 Intracranial haemorrhages of various types make it even more confusing. 8,9 There exist no less than 40 different systems to measure the severity or grade of head injury with little agreement between them. 10 Up to 80 per cent of patients that have suffered a traumatic brain injury may develop post-concussion syndrome 11 no matter how mild the original injury may have been. Recent research presented at the 4th International Consensus Conference on Concussion in Sports in 2012 suggested that re-peated mild traumatic brain injuries can result in cerebral atro-phy and long-term damage to the brain stem and corpus callosum known as chronic traumatic encephalopathy. 12 Figure 1: Clinical effects of laser therapy. of red and infrared light in the form of superluminous light-emitting diodes and laser diodes. The power output of these devices is below the level of surgical or other high-intensity lasers. Photon particles of light are absorbed by the mitochon-dria through cytochrome c oxidase and result in increased cel-lular ATP levels. 13 The neurometabolic cascade of concussion ultimately results in an inadequate supply of ATP to the dam-aged tissue. The ionic imbalance that results from this depleted ATP, can produce neuronal damage and cellular dysfunction. 14 LLLT, therefore has a unique opportunity to supply the brain with increased ATP production during a time when this help is most needed. In the case of neuropathic pain, LLLT has been proposed to mediate analgesia by releasing local neurotransmitters such as serotonin 15 , promoting the release of endorphins 16 and through its potent anti-inflammatory effect. 17 LLLT has been well docu-mented to stimulate tissue regeneration including angiogenesis, collagen production, muscle and nerve regeneration, cartilage production and even bone formation (See Figure 1). 13 In recent years, research in the field of LLLT has provided some promising pre-clinical evidence to support the use of this technology for the treatment of post-concussion syn-drome. In an animal model of acute TBI, mice treated with LLLT showed significant improvement in motor behaviour and reduction in mean lesion size. 18 In another animal model of moderate-to-severe TBI, mice treated with LLLT demon-strated significant improvement in the Neurological Severity Score in as little as five days post-treatment and continued to improve over the course of the follow-up, compared to sham-treated controls. 19 In humans, a number of individual cases have been doc-umented in which patients with chronic mild TBI showed marked improvement in cognition, executive function, mem-ory and sleep with light emitting diode (LED) treatments. 20 These patients may require continuing treatment to maintain and enhance these improvements. It is hypothesized that an overall protective response occurs with repeated LED treat-ment and that the therapy may reduce the oxidative damage and chronic inflammation that occurs in the brain following TBI, in addition to increasing cerebral blood flow. 18,19 The effects of trauma to the cervical spine are often over-looked. The brain stem extends through the atlanto-occipital junction and provides nerve connections between the motor and sensory systems from the central part of the brain to the entire body. It also regulates the central nervous system, and is www.canadianchiropractor.ca CONVENTIONAL TREATMENTS Depending on the severity of the injury, the treatment required may be minimal or may include interventions such as medi-cations and emergency surgery (decompression). Within the first few hours following injury, the primary aim of medical personnel is to stabilize the patient and focus on preventing further damage. While there is a tremendous focus on educa-tion for the prevention of concussion, there is minimal effort expended to reverse the damage caused by the initial trauma. Physical, speech and occupational therapy may be employed in the rehabilitation process, although complete recovery is not universally achieved in moderate or severe cases. Chiropractors have played a key role in the treatment of the musculoskeletal conditions that are often associated with these injuries, includ-ing whiplash, subluxation, neck strain, facet syndromes and muscle spasms. Current research shows that TBI symptoms and whiplash associated disorder (WAD) symptoms are very similar and may delay proper diagnosis and treatment. LASER MEDICINE fOR NEUROLOGICAL CONDITIONS For more than 40 years, Low Level Laser Therapy (LLLT) has been effectively used in the treatment of acute and chronic con-ditions, including degenerative disc disease, repetitive stress injuries, muscle strains, sprains and arthritis. 13 LLLT is a non-invasive, pain-free, light-based therapy that uses a combination 16 • CANADiAN CHiROPRACTOR | APRiL 2013
Chiropractic + Naturopathic Doctor April 2013: Page 16