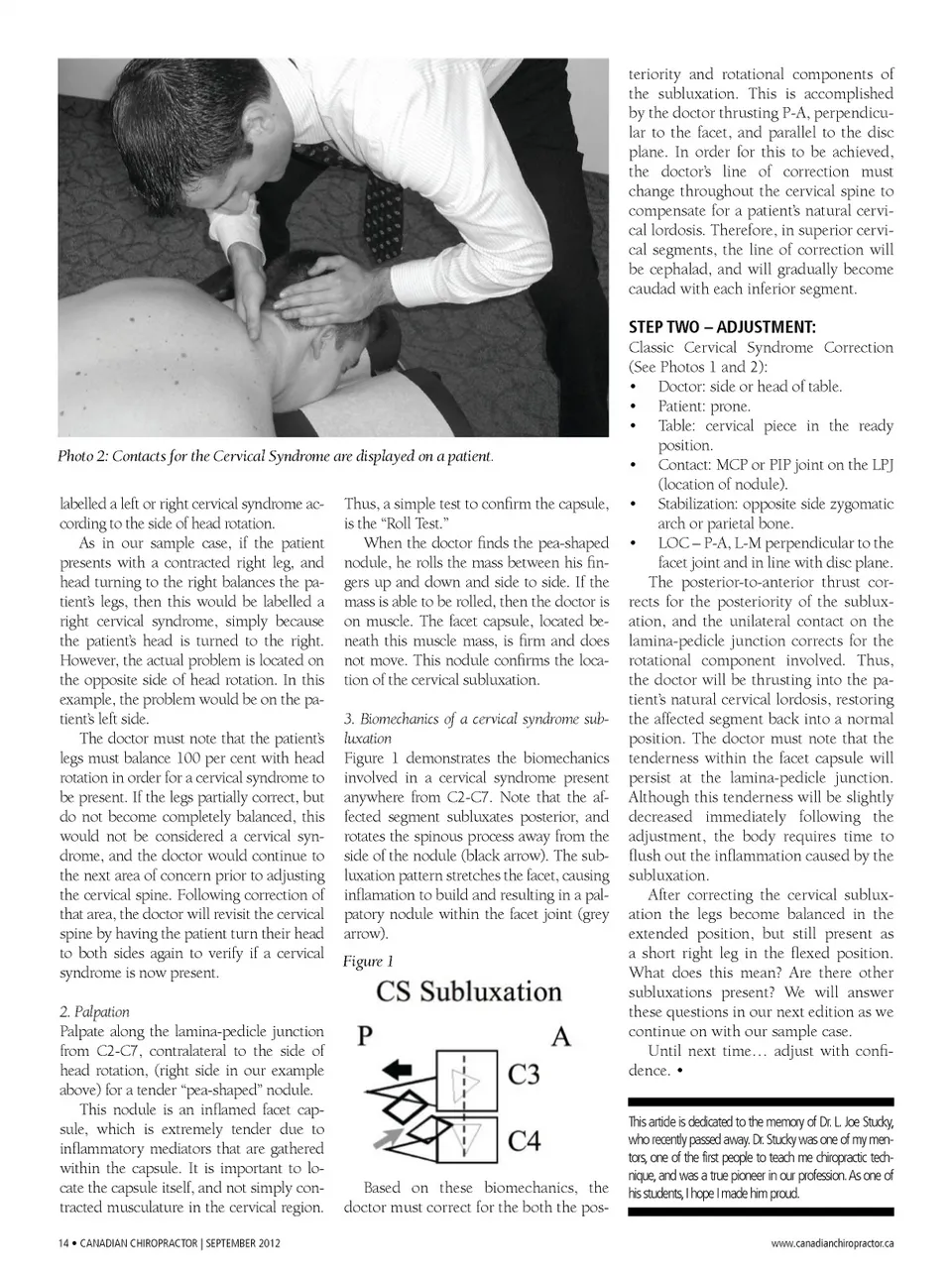
teriority and rotational components of the subluxation. This is accomplished by the doctor thrusting P-A, perpendicu-lar to the facet, and parallel to the disc plane. In order for this to be achieved, the doctor’s line of correction must change throughout the cervical spine to compensate for a patient’s natural cervi-cal lordosis. Therefore, in superior cervi-cal segments, the line of correction will be cephalad, and will gradually become caudad with each inferior segment. Photo 2: Contacts for the Cervical Syndrome are displayed on a patient. labelled a left or right cervical syndrome ac-cording to the side of head rotation. As in our sample case, if the patient presents with a contracted right leg, and head turning to the right balances the pa-tient’s legs, then this would be labelled a right cervical syndrome, simply because the patient’s head is turned to the right. However, the actual problem is located on the opposite side of head rotation. In this example, the problem would be on the pa-tient’s left side. The doctor must note that the patient’s legs must balance 100 per cent with head rotation in order for a cervical syndrome to be present. If the legs partially correct, but do not become completely balanced, this would not be considered a cervical syn-drome, and the doctor would continue to the next area of concern prior to adjusting the cervical spine. Following correction of that area, the doctor will revisit the cervical spine by having the patient turn their head to both sides again to verify if a cervical syndrome is now present. 2. Palpation Palpate along the lamina-pedicle junction from C2-C7, contralateral to the side of head rotation, (right side in our example above) for a tender “pea-shaped” nodule. This nodule is an inflamed facet cap-sule, which is extremely tender due to inflammatory mediators that are gathered within the capsule. It is important to lo-cate the capsule itself, and not simply con-tracted musculature in the cervical region. 14 • Canadian ChiropraCtor | SEptEMBEr 2012 Thus, a simple test to confirm the capsule, is the “Roll Test.” When the doctor finds the pea-shaped nodule, he rolls the mass between his fin-gers up and down and side to side. If the mass is able to be rolled, then the doctor is on muscle. The facet capsule, located be-neath this muscle mass, is firm and does not move. This nodule confirms the loca-tion of the cervical subluxation. 3. Biomechanics of a cervical syndrome sub-luxation Figure 1 demonstrates the biomechanics involved in a cervical syndrome present anywhere from C2-C7. Note that the af -fected segment subluxates posterior, and rotates the spinous process away from the side of the nodule (black arrow). The sub-luxation pattern stretches the facet, causing inflamation to build and resulting in a pal-patory nodule within the facet joint (grey arrow). Figure 1 STEP TWO – ADJUSTMENT: Classic Cervical Syndrome Correction (See Photos 1 and 2): • Doctor: side or head of table. • Patient: prone. • Table: cervical piece in the ready position. • Contact: MCP or PIP joint on the LPJ (location of nodule). • Stabilization: opposite side zygomatic arch or parietal bone. • LOC – P-A, L-M perpendicular to the facet joint and in line with disc plane. The posterior-to-anterior thrust cor-rects for the posteriority of the sublux-ation, and the unilateral contact on the lamina-pedicle junction corrects for the rotational component involved. Thus, the doctor will be thrusting into the pa-tient’s natural cervical lordosis, restoring the affected segment back into a normal position. The doctor must note that the tenderness within the facet capsule will persist at the lamina-pedicle junction. Although this tenderness will be slightly decreased immediately following the adjustment, the body requires time to flush out the inflammation caused by the subluxation. After correcting the cervical sublux-ation the legs become balanced in the extended position, but still present as a short right leg in the flexed position. What does this mean? Are there other subluxations present? We will answer these questions in our next edition as we continue on with our sample case. Until next time… adjust with confi-dence. • This article is dedicated to the memory of Dr. L. Joe Stucky, who recently passed away. Dr. Stucky was one of my men-tors, one of the first people to teach me chiropractic tech-nique, and was a true pioneer in our profession. As one of his students, I hope I made him proud. www.canadianchiropractor.ca Based on these biomechanics, the doctor must correct for the both the pos-
Chiropractic + Naturopathic Doctor September 2012: Page 14